As many readers know, HIV also disproportionately affects LGBTQIA+ people – it was once referred to as the “gay plague” during its early years when thousands of queer people were being killed each year while government-funded research facilities pushed the harmful belief that HIV was a divine punishment ordained by God. All marginalized groups are at higher risk of contracting HIV, culminating from a lack of educated doctors, accessible testing, preventative medicine like PrEP and PEP, and public knowledge. Ultimately, this means that young queer people are at an exceptionally higher risk of HIV – especially transgender youth of color.
Despite heightened rates reported by the CDC, they also found that only 6% of high school students had ever been tested for HIV. Most people are never offered an HIV test when visiting a healthcare provider’s office – there’s often very little signage and educational material present advertising HIV prevention and its risk and even fewer offices discuss HIV with their patients unless they believe they’re a ‘high risk.’ Unfortunately, this process is based on stereotypes even among healthcare providers well-educated on HIV versus reality – so lots of folks fall through the cracks. The CDC recommends all individuals, regardless of sexual orientation, gender identity, age, class, race, ethnicity, or background, be tested for HIV at least once in their life. Certain people are advised to be tested regularly based on their sexual activity – as a general note, the CDC says the following people should be tested for HIV at least once per year:
Men who have had sex with other men.*
Individuals who have had anal or vaginal sex with someone who is living with HIV.
Individuals who have had sex with more than one partner since their last HIV test.
Drug users who share injection equipment, like needles, syringes, and cookers.
Individuals who have had sex for money, drugs, or housing.
Individuals who have been diagnosed with another STD/STI, hepatitis, or tuberculosis.
Anyone who has had sex with someone who has done one of the above things or you’re unsure about their sexual history.
In February 2025, the Trump administration tried to remove mentions of LGBTQIA+ people from official government websites – including the CDC. Federal courts have rebuked this decision as purposeful misinformation of scientific research and forced the administration to restore previous web pages, although they have altered some of the sites and added a political anti-science disclaimer stating the agency denounces transgender people alongside the Trump administration.
All governmental information and research regarding HIV was targeted by this purge – I’m unsure whether the first statement was present before the restoration since it’s not aligned with current HIV advocacy and data. Most organizations disagree with blanket stereotypes for HIV and testing based on sexuality, instead pushing for non-discriminatory testing requirements based on sexual activity. This can be seen in the change in the Red Cross’s policies allowing queer men to finally donate blood after decades of permanently banning them for “having had sex with men” since data shows such practices do not effectively reduce HIV risk during blood donation.
HIV 101: The Basics
In today’s world, most people have a basic understanding that HIV exists, that it’s an STD, and it disproportionately targets queer men. Other than that, knowledge varies drastically since HIV isn’t covered in many public school sexual education programs (and several states don’t have sex ed) and most healthcare providers do not bring up HIV unless they believe they have enough reason to do so.
As mentioned earlier, anyone can be affected by HIV – the virus doesn’t discriminate based on sexual orientation, gender identity, race, ethnicity, age, class, education, religion, neighborhood, etc. There is no singular way to ‘tell’ if someone has HIV other than getting tested: most people don’t experience symptoms until HIV has developed into AIDS years later. Lastly, HIV won’t kill you – while living with HIV will greatly change your life, people live long, happy, and fulfilling lives with HIV when taking prescribed medication to treat the virus.
Want to learn more about HIV?Read this post here or check out one of the sources below.
Education is crucial.Teaching youth about HIV and safe sex is the first step in reducing the spread of STDs, including HIV. Despite this reality, many schools, politicians, and religious figures argue that comprehensive sex education encourages young people to have sex. This is fallacious – data shows that folks will have sex regardless, but it is possible to reduce STDs and unplanned pregnancies by giving them the tools to have safe and healthy relationships.
Accessibility is just as important. Most people know what they ought to do, whether it’s safe sex or recycling plastic. However, they’re unlikely to do it unless it is convenient – it’s human nature. Convenient testing is offered at regular healthcare visits, community centers, and even social events like local drag shows and pride events. Some organizations offer incentives for testing like free entry to an event, gift cards, vouchers, or coupons to engage folks in testing when they may otherwise be too hesitant. Making condoms free and easy to access discreetly without shame encourages people to practice safe sex. Preventative medicines like PrEP and PEP are most impactful when folks have access to those medicines when they need them – whether it’s by visiting a local pharmacy or getting it mailed directly to their house.
Where do I get tested for HIV?
You can only get treatment for HIV if you’ve tested positive, which requires you to get tested in the first place – so seeking testing is the first step to protecting your health. The earlier someone gets diagnosed, the sooner they can access life-saving treatments to manage their HIV.
Greater Than (linked above) is one of the largest public health campaigns in the United States that provides detailed resources in partnership with the CDC. Click above to be redirected to their website, which locates HIV testing, PrEP providers, and support services locally by zip code. Greater Than also connects individuals to health insurance information to educate users on state laws dictating coverage.
IRL testing isn’t for everyone – that’s why the CDC also sponsors the Together TakeMeHome program to ship free HIV tests directly to homes throughout the United States. These tests are done via an oral swab with saliva to give results within 20 minutes, and the program provides two free tests to individuals every 90 days. Together TakeMeHome has been providing free tests since early 2023, so click the button below to learn more about how to use their services.
Together TakeMeHome is currently operating, although it can only do so through government funding. Due to the current political climate and attacks by the Trump administration on other HIV programs, it’s not impossible to consider the possibility that the program could be shut down in the future. Most LGBTQIA+ community centers also provide HIV testing for free, and many cities offer similar programs to Together TakeMeHome with mail programs to increase HIV testing in their area.
Know Your Rights: Young People, HIV, and the Law
In the United States, all individuals with HIV are protected by the Rehabilitation Act of 1973 and the Americans with Disabilities Act of 1990, which is enforced by the Department of Health and Human Services and the Office for Civil Rights. These laws prohibit any anti-HIV discrimination by healthcare and human services agencies that receive federal funding, as well as any discrimination by state or local governments – including services, activities, or programs provided by state or local governments. Anyone can file a report with the Office for Civil Rights online or by mail.
In all US states, minors have the right to consent to HIV and STD testing and treatment without a guardian’s permission. Generally, youth have the right to get tested (and receive HIV medication) without telling their parents. However, these laws vary on whether you have the right to access preventative services like PrEP without parental consent. There are no state or federal laws that explicitly prohibit minors from accessing PrEP, but you should search for laws specific to your state for details.
Many states don’t have health confidentiality protections for minors, so it’s extremely likely for your guardian to find your status if you get tested at your primary provider – especially if your doctor bills your family’s insurance company for the test. For this reason, many LGBTQIA+ community centers provide free confidential HIV testing to encourage youth to get tested without fear that their authority figures will discover they got tested.
While many US states and territories require you to disclose your HIV status, you’re only required to disclose it to certain people. At the time of this article, thirteen states require you to disclose your status to potential sexual partners, while four require disclosure to anyone you share a needle with.
Depending on the state, failure to disclose status can lead to life in prison. You do not have to disclose to anyone else – including your family or friends. While most American employers have the right to ask about your health in certain fields, you don’t have to disclose it to your workplace in most cases. The Americans with Disabilities Act protects you from anti-HIV discrimination – which means hiring managers can’t ask you about your health and companies have to make reasonable adjustments as needed. These protections also apply within education, so you’re not required to disclose your HIV status to anyone at school unless you reside in a state requiring disclosure for potential sexual partners or needle sharing.
AIDS Drug Assistance Program@ adap.directory / Patient-centric project that provides HIV-related services and prescription medication to hundreds of thousands of people in the United States by linking individuals with their local state or territory agency.
AIDS Healthcare Foundation @ aidshealth.org / 323-860-5200 / International nonprofit based in Los Angeles that operates a network of HIV services in over 40 countries across Latin America, Africa, Asia, and Europe.
Asian Pacific AIDS Intervention Team @ apaitssg.org/ Grassroots AIDS service organization centered on Asian and Pacific Islanders with HIV, based in the United States.
Bienestar Human Services @ bienestar.org / US community-based social services organization that caters to Latino Americans living with HIV, especially LGBTQIA+ Latino Americans.
Black AIDS Institute @ blackaids.org / Think tank that aims to end the HIV/AIDS epidemic in the Black American community through awareness messaging, information, and robust programs.
CDC-INFO @ cdc.gov / 800-232-4626 / Live support to help Americans find the latest and reliable science-based health information, including CDC guidance and resources.
Global Network of People Living with HIV @ gnpplus.net / Network operated by people living with HIV for people living with HIV, regardless of geographic location.
HIV/AIDS/Hepatitis C Nightline / 800-273-2437 / US hotline providing support for people living with HIV or Hepatitis C as well as their caregivers.
HIV. GOV @ hiv.gov / Offers information about HIV/AIDS prevention, treatment, and resources for anyone in the United States.
HIV.GOV Service Locator @ locator.hiv.gov / Location-based search tool managed by the United States Department of Health and Human Services to allow anyone to find local HIV testing services, housing providers, health centers, PrEP, PEP, and other related needs.
HIV Management Warmline / 800-933-3413 / Non-emergency telephone service for questions about HIV, antiretroviral therapy, HIV clinical trials, and laboratory evaluation in the United States.
International AIDS Society @ iasociety.org / Research-based organization that develops holistic approaches to HIV/AIDS treatment and prevention.
International Planned Parenthood Federation @ ippf.org / 202-987-9364 / Global healthcare provider that has been a leader in sexual and reproductive health for all since 1952.
Latino Commission on AIDS @ latinoaids.org / Nonprofit organization in response to the critical unmet need for HIV prevention, treatment, and education in the Latino community in the United States.
LGBT National Help Center @ lgbthotline.org / 888-843-4564 /Free and confidential peer support, information, and local resources where volunteers help connect you to other groups and services in the US. Also maintains a coming out hotline, youth talkline, and senior hotline.
National AIDS Hotline / 800-243-2437 / Federal hotline to refer the general American public to relevant state and local resources.
National AIDS Treatment Advocacy Project @ natap.org / 212-219-0106 / Nonprofit corporation in the United States that educates individuals on HIV treatments on the local, national, and international levels.
National Clinician Consultation Center @ nccc.ucsf.edu / 833-622-2463 / Teleconsultation resource that educates US healthcare providers with information and answers on HIV and Hepatitis C.
National Minority AIDS Council @ nmac.org / Advocacy nonprofit that provides training and resources catered to marginalized communities in the United States.
National Native HIV Network @ nnhn.org / Indigenous-led network that mobilizes American Indians, Indigenous Americans, Alaska Natives, and Native Hawaiians towards community action.
NIH Office of AIDS Research @ hivinfo.nih.gov / 800-448-0440 / Confidential answers to questions on HIV/AIDS clinical trials and treatment in the United States.
PEPline / 888-448-4911 / Hotline for individuals interested in information about PEP, especially those who have been possibly exposed to HIV while on the job in the United States.
Perinatal HIV Hotline / 888-448-8765 / Resource hotline available 24/7 in the United States for pregnant people living with HIV to find answers and tools.
Positively Trans @ transgenderlawcenter.org / Program through the Transgender Law Center to support transgender people living with HIV in the United States.
Positive Women’s Network @ pwn-usa.org / Advocacy and resource organization for women living with HIV.
PrEPline / 855-448-7737 / Hotline about how to start, continue, or manage use of PrEP for HIV within the US.
Ryan White HIV/AIDS Program @ ryanwhite.hrsa.gov / National services and resources for low-income individuals living with HIV in the US.
TheBody.com Hotline @ thebody.com / News site based in New York that centers on publishing HIV-related information.
The Trevor Project @ thetrevorproject.org / 866-488-7386 / The leading suicide prevention and crisis intervention organization centered on LGBTQIA+ young people in the United States. Offers 24/7/365 information and support to those ages 13 to 24 with trained counselors via call, text, or instant message.
The Well Project @ thewellproject.org / United States nonprofit that primarily supports women and girls living with HIV/AIDS.
Trans Lifeline @ translifeline.org / 877-565-8860 / Transgender-centered crisis organization that does not use involuntary intervention/forced hospitalization to provide support to transgender people through fully anonymous and confidential calls within the United States and Canada.
UNAIDS @ unaids.org/ 41-22-595-59-92 / International agency that seeks to end AIDS as a public health threat by 2030 and has operated since 1996 to assist the United Nations in combating HIV and AIDS.
Reproductive health is more than just abortion – it’s also preventative primary care, birth control, cancer screenings, fertility treatments, and safe access to abortion procedures. The right to one’s body, or autonomy, is tied to reproductive healthcare and gender-affirming services. Despite the shame and hate tied to these fields, few services are linked to human rights and equality worldwide.
Looking for general information about non-reproductive medical healthcare or health insurance?Click here.
Bodily autonomy is tied to certain laws around the world, like age, ability, or gender. In the United States, children are denied bodily autonomy for most medical decisions until they turn 18 – they’re only able to see a medical provider under their parent’s supervision and decision rather than their own. Likewise, disabled people of any age are generally denied bodily autonomy – so it’s not uncommon for disabled people to be denied the ability to marry or have sex because other people like their parents or guardians get to make that decision for them. In countries like South Sudan, women are denied the bodily autonomy to deny or reject marriage (or get divorced) since their families make those decisions on their behalf. Likewise, in places like Egypt, transgender people are denied the bodily autonomy to gender-affirming care such as hormone replacement therapy.
Author’s Note: All aspects of reproductive health and gender-affirming care are rather unstable due to the national political stage. It’s unlikely (but not impossible) for a nationwide ban on care, but it is likely for national protections to be removed – making it difficult to find abortion or gender-affirming care in hostile states.
Looking for more resources?
Browse Trans Solidarity Project’s resources, or check out these posts:
Contraception is the technical term for “birth control,” which is any medication, device, or surgery that prevents pregnancy. Birth control techniques can be temporary, reversible, or permanent – and a few also prevent sexually transmitted diseases (STDs).
They achieve this by killing sperm, making a physical barrier between the sperm and egg, preventing eggs from being released in the ovaries, and altering the uterus tissue so fertilized eggs can’t be implanted.
Types of Birth Control
IUDs
Intrauterine devices(commonly referred to as IUDs and IUCs) are one of the most effective kinds of birth control available. There are five main brands approved by the FDA for use in the United States: Paragard, Mirena, Kyleena, Liletta, and Skyla
Most IUDs are hormone-based and use the hormone progestin to prevent pregnancy, whereas Pargard is wrapped in copper to prevent pregnancy instead of hormones. Paragard IUDs prevent pregnancy up to 12 years, while hormone-based ones range from 3 to 8 years.
The reason Paragard works so well is that sperm naturally dislike copper. It’s a natural, non-hormonal deterrent that creates an internal barrier between the egg and sperm.
Progestin mimics the progesterone that bodies naturally make, which will either thicken the cervical mucus to physically block and trap sperm or prevent ovulation entirely.
IUDs are highly recommended for pregnancy prevention since they’re extremely low-maintenance, highly effective, long-lasting, and reversible. After being inserted by a medical provider, you’re covered by a 99% effectiveness rate until it’s removed. There are no daily pills to take, days to track, or mistakes to avoid.
YSK: Since copper-based IUDs don’t use hormones, they are a common choice among transmasculine people since they won’t interfere with gender-affirming care.
Implants
Birth controlimplants, or Nexplanon, are another highly effective and low-maintenance form of birth control that prevents pregnancy up to five years after it’s originally inserted.
Just like IUDs, implants release the hormone progestin to prevent pregnancy – but instead of being inserted in the cervix, the implant is placed in the upper arm. Compared to IUDs, implants aren’t associated with as much pain during insertion since numbing agents are used to ease the process.
Unfortunately, implants aren’t covered by as many government programs to be offered for free as IUDs.
Depo Shots
Depo shots are injections received once every three months – but unlike IUDs and implants, depo shots can occasionally be done at home without a doctor’s appointment.
Just like most IUDs and implants, birth control shots use progestin to prevent pregnancy. While shorter lasting, the shot doesn’t require anything to be implanted or inserted, BUT it must be taken every 12 to 13 weeks to remain effective. Birth control shots are easier to pay for out-of-pocket without insurance or government programs: an IUD can cost up to $1,800, one implant can range upwards of $2,300, but the shot costs $150 at most.
Vaginal Ring
Did you know birth control can also be taken as a vaginal ring? The birth control ring is a small, flexible ring placed inside the vagina to prevent pregnancy for up to a month at a time – which has some caveats.
The ring and other forms of birth control have lower effectiveness rates than IUDs and implants since they require more upkeep and are accident-prone. That being said, the ring is still 93% effective when used correctly. There are two main types of birth control rings:
NuvaRing is capable of stopping periods and is replaced every month. It lasts up to five weeks at most, so if you forget to replace it, you’re at risk of becoming pregnant.
Annovera rings are used for three weeks before being removed for seven days. After one ring-free week, the Annovera ring is re-inserted into the vagina. While NuvaRings have to be discarded each month, Annovera rings last one year each if used on schedule – but they don’t stop periods.
Both ring types prevent pregnancy by stopping ovulation through the use of estrogen and progestin, which is absorbed from the ring into the vaginal lining.
Like IUDs, implants, and the shot, a prescription is required – but unlike them, you have the freedom (and responsibility) to take the ring on your own time.
Patches
The birth control patch is another safe and convenient option, where a prescribed transdermal patch is worn on the skin to prevent pregnancy by releasing estrogen and progestin, just like traditional birth control pills.
The patch must be replaced weekly to be effective, and it only works if it’s stuck properly. This means no lotion, creams, powders, or makeup can be used near them, and you can’t be sensitive or allergic to the adhesive.
All forms of birth control that are taken on your own, such as the ring, patch, or pill, can be prescribed online by telehealth.
Pill
The most popular form of birth control today is the pill, a 93% effective oral medicine that prevents pregnancy if taken every day.
Once approved by the FDA in 1957, the pill had a profound effect on feminism and women’s sexual liberation since it was the first mainstream medicine that allowed them to choose motherhood.
Birth control is covered by nearly all American health insurance and welfare plans, and Opill has been the national form of birth control available over-the-counter without a prescription or doctor’s visit since 2024.
Other Birth Control Methods
Those aren’t the only options for birth control, either – some additional (but less common) forms include:
Cervical caps are soft silicone cups placed deep inside the vagina to cover the cervix, creating a physical barrier between sperm and the egg. A prescription is required and they’re around 71% to 86% effective – but they work even better when used with spermicide. Smaller than the diaphragm, cervical caps can be left for up to two days before being removed.
Diaphragms are soft silicone cups that are bent and then inserted into the vagina to cover the cervix, creating a physical barrier to stop pregnancy. Like cervical caps, a prescription is required for diaphragms. They can’t be left inside the vagina as long as caps, but they’re generally more effective (83%) since they don’t have the larger range caps do. Similar to cervical caps, diaphragms work best when used with spermicide.
Contraceptive sponges are made from soft, squishy plastic that’s placed inside the vagina before sex to cover the cervix, creating a barrier to prevent sperm from reaching the egg and causing pregnancy. Sponges vary from 78% to 86% effective and need spermicide to work best – but unlike cervical caps and diaphragms, contraceptive sponges don’t require a prescription.
Spermicide and contraceptive gels contain chemicals that stop sperm from reaching the egg, placed inside the vagina before sex. It ranges from 79% to 86% effective at preventing pregnancy and doesn’t require a prescription – it’s found over-the-counter at most drugstores, pharmacies, and supermarkets. However, spermicides don’t work on their own; you have to use a diaphragm or cervical cap alongside it.
Condoms
Condoms are thin pouches that create a physical barrier between genitals during sex, and they’re the only option that prevents both pregnancy and sexually transmitted diseases.External or male condoms are worn on the penis, collecting semen and preventing sperm from reaching the egg. Internal or female condoms are worn inside the vagina or anus, similarly collecting semen.
Condoms must be worn every time you have sex to be effective.
Always check the expiration date before use.
Look for potential tears.
Never store condoms in hot or cold places or direct sunlight.
Double-layering condoms increases the risk of a tear or breakage, not protection.
Latex
Most condoms are made of latex rubber, which can be found in any supermarket, pharmacy, online, or at health centers. They’re also the cheapest, so they’re offered for free at many organizations.
Latex condoms can only be used with water and silicone-based lube – oil-based lubricants can damage latex condoms. Note that silicone-based lube can damage silicone toys and prosthetics, so check your items prior to use.
Plastic
Plastic condoms are made from materials like polyurethane, nitrile, and polyisoprene to create an alternative that’s better suited for individuals with latex allergies. Plastic condoms are more expensive than their latex counterparts, so they’re not as commonly found in some regions.
Water and silicone-based lube is best suited for plastic condoms, although oil-based lube can be used for any plastic condom not made from polyisoprene.
Internal condoms are made from plastic, not latex – so the same rules apply. Latex and animal skin condoms are not options for female condoms.
Lambskin
Lambskin and animal skin condoms are made from the lining of the intestines, but they’re only able to prevent pregnancy.
Compared to other condom alternatives, animal skin condoms don’t prevent STDs due to the materials used. Unlike other condoms, lambskin condoms can be used safely with any type of lube.
Experts advise regular use of both condoms and birth control for sexually active individuals at risk of pregnancy. In relationships where pregnancy isn’t possible, condoms and/or PrEP should still be used since STDs don’t discriminate against gender identity or sexual orientation.
Outercourse can prevent pregnancy, but it can’t prevent STDs. Remember to wear a condom if STDs are a potential risk.
Some people purposely don’t have sex or become temporarily abstinent when they’re at risk of becoming pregnant based on their menstrual cycle. This is called “natural family planning,” “the rhythm method,” and fertility awareness methods (FAMs). It requires a higher level of dedication since it’s your personal responsibility to track ovulation.
Pull-Out Method
In a similar vein, some individuals practice the withdrawal method as their primary form of birth control – also referred to as pulling out. By pulling out the penis from the vagina before ejaculation (or cumming), pregnancy can be prevented since sperm is physically kept from the egg.
Pulling out only works when done correctly before ejaculation since any amount of semen (no matter how little) can cause pregnancy if inside the vagina. It doesn’t prevent STDs, and it’s notoriously difficult to do correctly – leading it to have lower efficacy rates than other birth control methods.
YSK: One large reason condoms and birth control practices like those mentioned above are considered best is that pregnancy and STDs can also occur from precum, meaning before ejaculation.
While the chances are low, it is possible to become pregnant from precum since sperm mixes with the alkaline fluid in the urethra. In other words, pregnancy can still happen even when you perform the withdrawal method perfectly since just one viable or healthy sperm is needed to fertilize an egg.
Lactation
The last non-permanent form of birth control is breastfeeding since regular breastfeeding stops the body from ovulating and therefore prevents pregnancy. It’s also called the lactational amenorrhea method (LAM) because it also naturally stops the period and works at similar rates as oral birth control pills.
LAM only works if you’re breastfeeding, which requires you to have recently been pregnant.
Permanent Sterilization
There are two main types of permanent birth control, referred to as sterilization. They are 99% effective at preventing pregnancy (but not STDs).
These are not reversible and considered life-long decisions, which is why they can be difficult to access since the economy and government have a weighted interest in forcing young people to have children. On the other hand, certain groups of individuals have been targeted for forced or coerced sterilization like women of color, disabled people, and transgender people.
Tubal Sterilization
Individuals assigned female at birth can undergo tubal sterilization (“getting the tubes tied”). There are three subtypes of tubal ligation, which all physically prevent sperm from reaching a viable egg by blocking or removing the fallopian tubes.
Tubal ligation surgically closes, cuts, or removes pieces of the fallopian tube.
Bilateral salpingectomy removes the fallopian tubes entirely.
Essure sterilization uses a tiny coil to block the fallopian tube – while it used to be a common form of sterilization, essure sterilization is no longer available in the United States.
Vasectomy
Individuals assigned male at birth can opt for a vasectomy, a procedure where the small tubes inside the scrotum are cut or blocked that carry sperm.
Incision vasectomy utilizes one or two small cuts on the vas deferens by tying, blocking, cutting, or closing with electrical currents. It is an extremely fast procedure that takes about 20 minutes before it’s stitched up.
No-scalpel vasectomy requires the doctor to make one small puncture to both of the vas deferens tubes before tying off, blocking, or cauterizing the tubes. Since the skin isn’t cut with a scalpel, there’s no need for stitches or scarring and it heals quickly.
Accidents Happen: Emergency Contraception
Birth control prevents pregnancy ahead of sex, relying on the various methods above to be used before/during sex. In contrast, emergency contraception prevents pregnancy after sex- most EC is 95% effective up to five days after unprotected sex (as well as other reasons for emergency contraception like contraception failure, incorrect use of birth control, or assault).
Emergency contraceptive works by temporarily stopping the body from releasing an egg, preventing ovulation that puts you at an increased risk of pregnancy. Pregnancy doesn’t happen immediately after sex nor does it happen every time you have sex – that’s why EC works and why it is different from abortions.
IUDs as Emergency Contraception
IUDs are more than just birth control: they’re considered one of the most effective forms of EC. Unlike other emergency contraceptives, IUDs don’t decrease in efficiency if taken within five days.
They’re just as effective at preventing pregnancy on day five as they are on day one. And as an add-on, IUDs aren’t weight-based and work for all body sizes. On the downside, it’s more difficult to get an appointment for an emergency IUD compared to the following EC pills.
Morning After Pill
There are two types of “morning-after pills,” which are the more commercially available forms of emergency contraception available for purchase. It is important to note that emergency contraceptive pills work best when taken as soon as possible after sex because their effectiveness decreases with time, even if you’re within the appropriate five-day span.
Ulipristal acetate-based pills (brand name Ella) are the most effective EC pills but require a prescription. It can be taken up to 120 hours after sex and works best for individuals who weigh 195 pounds or less.
YSK: All forms of morning-after pills don’t work if you’re already ovulating. Ella is capable of working closer to ovulation, but an IUD may be a better EC option if you’re ovulating.
Levonorgestrel-based pills (brand names Plan B, Take Action, My Way, Option 2, AfterPill, etc.) are available over the counter at any drugstore, pharmacy, or supermarket. It should be taken within 72 hours after sex and works best for individuals weighing 165 pounds or less. However, it’s not uncommon for people who weigh more to take an additional dose.
There’s a lot of misinformation about Plan B and its variants. Since 2013, there hasn’t been an age requirement to buy Plan B over-the-counter – regardless of where you are in the United States. Some stores may lock Plan B in security packaging to deter theft, but it can be purchased at any time of the day and cannot be restricted if the store is open. No IDs are necessary to buy Plan B, either.
Under the Affordable Care Act, most commercial insurance plans fully cover Plan B as well as government alternatives like Medicaid. However, having insurance or Medicaid pay for Plan B requires a prescription.
Out of pocket, Plan B costs about $40 over the counter. Pro-tip: It’s significantly cheaper to buy Plan B ahead of a crisis, like via Amazon, but it will take longer to arrive while it ships.
Part of the reason Plan B can sell so high is due to demand, since $40 is still significantly less than the cost of having a baby. There are also select organizations and programs that provide Plan B for free, although their supply is limited.
Emergency contraceptive pills are considered extremely safe. They’ve been around for over 30 years and haven’t had any reports of serious complications. EC doesn’t have any long-term side effects and won’t have any impact on your ability to potentially get pregnant in the future.
It is not advised to use two different kinds of morning-after pills at the same time, such as Ella and Plan B. By doing so, they may counteract and not work at all.
Emergency contraceptives shouldn’t be used in place of regular birth control methods. While it’s safe to take EC pills multiple times as needed, it’s not as effective at preventing pregnancy – it’s also significantly more expensive.
Health is a state of complete physical, mental, and social well-being, which includes reproductive wellness. Nearly all of the clinics and organizations that provide abortion services and birth control also offer in-depth services for reproductive health, which is why entities like Planned Parenthood are important.
Reproductive healthcare refers to the services provided to support one’s physical, mental, and social well-being concerning one’s reproductive system. Most diseases are preventable or treatable if caught early, so seeing a healthcare provider regularly is critical to staying healthy.
STDs & Preventive Testing
Everyone should see a provider annually for screenings best suited for their age and health. All sexually active people should be tested every three to twelve months, depending on their risk factors.
Sexually transmitted infections (STIs) and diseases (STDs) spread during vaginal, anal, oral, and blood-to-blood contact. All STDs are treatable, and most are completely curable – but only if you get care from a healthcare professional.
STDs can be tested through blood samples, urine tests, saliva swabs, spinal tabs, and visual examinations. It varies by jurisdiction, but most US states allow people ages 13 and older to be tested and treated for STDs without parental consent.
Vaccines exist to prevent STDs like hepatitis B and HPV, which are given to most children in the United States around age 11 or 12. These vaccinations are recommended for all young people regardless of gender since these illnesses do not discriminate based on gender.
Regular self-exams are necessary in order to know what your “normal” is. Everybody is unique and covered in various lumps and bumps, so self-examining your body lets you know when something is potentially wrong and worth professional attention.
People of all genders should know what their breast tissue normally feels like through breast self-exams (BSEs). Everyone, including cisgender men, has breast tissue – which is capable of producing cancer. Individuals with a high family risk of breast cancer as well as all women 40 or older are recommended to get mammograms, which can detect cancer in its earliest stages when it’s most curable.
Folks with uteruses need to get pelvic or internal exams once they turn 21 years old, which requires a doctor’s visit where a professional examines the vulva, vagina, cervix, ovaries, fallopian tube, and uterus. Pelvic exams are recommended annually, whereas pap smears (which are different from pelvic exams) are advised every three years to check for early signs of cervical cancer.
Individuals with testicles need to do a testicular self-exam (TSE) at least once a month at age 15. That’s much younger than most people realize or what most public schools teach, but AMAB individuals are at the greatest risk of testicular cancer from the ages of 15 to 35.
People with prostates get prostate or rectal exams when there’s an issue with the anus, prostate itself, or constipation. Younger folks only get prostate exams if there’s a cause or concern, but anyone with a high risk of prostate cancer or age 55 or older is recommended to get a prostate exam annually.
Infertility
Infertility is characterized as the inability to cause a pregnancy despite regular unprotected sex. The World Health Organization estimates that 17.5% of adults experience infertility issues, which translates into 1 in 6 adults.
Healthcare providers can perform semen analysis, hormone testing, genetic testing, thyroid testing, biopsy, imaging, hysterosalpingography, and other methods to determine if someone is experiencing infertility.
YSK: Hormone replacement therapy can have long-lasting and permanent effects on fertility among transgender people. While puberty blockers do not affect fertility, the use of HRT can make someone incapable of having biological children later in life.
Aspiring transgender parents can freeze sperm and eggs for future use. Temporarily pausing HRT can improve fertility, although it generally believed that the longer someone is on HRT, the more likely they will become infertile.
Infertility for individuals assigned male at birth revolves around a lack of healthy sperm. Men are prescribed lifestyle changes as a first step to resolving infertility, although lifestyle and habits play a significant role in anyone’s fertility, regardless of gender.
Some of these prescribed habits include more frequent sex, increased exercise, diet changes, and stopping alcohol and nicotine use alongside other substances. While many of these are manageable, some lifestyle impacts are difficult to control – like one’s exposure to radiation or pesticides in their environment or neighborhood, which is known to cause infertility.
Half of male infertility cases have no determined cause. It’s a complex issue that can be influenced by countless factors like genes, hormones, and lifestyle.
Age 40 is the general guideline when cisgender men are expected to become naturally less fertile. The decrease in fertility is relatively insignificant at 40, although it gradually increases with age.
Unresolved sexually transmitted diseases contribute to male infertility since STDs like chlamydia and gonorrhea are notorious for doing so.
Physical blockages can naturally occur. Surgery can be performed to reverse the blockage and restore fertility.
Some medications impact fertility. Several medicines promote male fertility, which often boost testosterone levels and lower estrogen levels as a means to promote sperm production. However, synthetic testosterone does not help with male infertility. The medical consensus is that synthetic testosterone lowers male fertility rates.
Doctors may recommend assisted reproductive techniques like artificial insemination. Individuals produce a semen specimen to be processed, drastically increasing the concentration of healthy sperm before it’s placed into a uterus before ovulation. While IVF is more popular with lesbian same-sex couples, other assisted reproductive techniques include cryopreservation and surrogacy, which is employed by many gay same-sex couples otherwise unable to have biological children.
Individuals assigned female at birth can also experience infertility issues. The same lifestyle changes suggested for men can also promote female fertility, such as bettering nutrition and quitting cigarettes.
Between 20% to 30% of female infertility causes have no established cause, although this estimate fluctuates by source.
There’s more misinformation regarding female infertility and age, especially since there is an economic interest in having women pay for fertility treatments. 35 is the estimated age when female fertility begins to decline – but it’s a gradual continuum like men’s fertility.
Language like “geriatric pregnancy” purposely tries to scare women into having children young, even if they’re unsure about parenthood. One of the largest studies on the subject found 73% of women between the ages of 34-40 naturally conceiving within one year of regular sex at least twice a week. That’s not much lower than the 88% of women aged 30-34 or the 84% of women between 25-29.
Pelvic inflammatory disease (PID) is a complication associated with untreated STDs that damage and scar the fallopian tubes, leading to infertility since it obstructs the egg from traveling to the womb for fertilization.
Hormone and ovulation issues are the most associated with female infertility since conditions like polycystic ovary syndrome (PCOS) and thyroid-related diseases prevent ovulation. Both an overactive and an underactive thyroid gland prevent ovulation.
While ovulating, the cervix naturally produces thinner mucus to allow sperm to swim more easily. Some female fertility issues stem from problems with the cervical mucus itself, since it can make it harder to conceive.
Non-cancerous growths called fibroids can affect fertility, especially when they’re in or around the womb. Endometriosis is also associated with female infertility, eventually damaging the ovaries and fallopian tubes. Hysteroscopy and related surgeries can improve fertility by removing scar tissue, polyps, and fibroids, while laparoscopic surgery can treat large fibroids and infertility caused by endometriosis.
Certain medications have negative impacts on fertility, like non-steroidal anti-inflammatory drugs (NSAIDs), neuroleptic drugs, and other substances. There are several medications used to promote female fertility, like clomiphene citrate, gonadotropins, metformin, letrozole, and bromocriptine.
The assisted reproductive technique recommended for women is in vitro fertilization (IVF), although this procedure is continually under attack by religious conservatives in America. During IVF, eggs are taken from the ovaries to be fertilized by sperm in a lab – after they’ve developed into embryos, they’re placed into the uterus to resume pregnancy. IVF is especially popular with same-sex couples alongside surrogacy and egg/embryo donation.
Prenatal Care
Reproductive healthcare also includes prenatal care, which refers to the specialized services given during pregnancy to promote both the health of the pregnant person and the baby. Without prenatal care, it’s impossible to know the pregnancy is staying on track and ensure the baby is healthy, which is why ultrasounds and testing are used to gauge health.
Tests like amniocentesis check for certain birth defects, while chorionic villus sampling tests for genetic abnormalities that can happen during pregnancy.
It takes more than just one doctor to ensure a healthy pregnancy – doulas are non-medical professionals trained to guide a pregnant person and their family.
The use of a companion during childbirth dates back to prehistoric times, and doulas provide support with childbirth, miscarriages, induced abortions, stillbirth, and death. Similarly, midwives are medical professionals who can provide care and medicine to pregnant people, new mothers, and newborns.
Midwives are used for ultrasounds and are best for monitoring the progress of labor – the defining difference between midwives and doulas is that doulas provide more emotional support but are unable to practice medicine like certified midwives.
Abortions are Healthcare
One-quarter of women will have an abortion by age 45 for a variety of reasons – like already having children, health issues, money, being in school, not wanting kids, etc. There’s no singular reason, and they’re all valid reasons to not want to pursue parenthood. Abortions are medical procedures that terminate a pregnancy.
Mifepristone and misoprostol pills are effective at terminating pregnancies that are at ten weeks or fewer, forcing the body to expel the pregnancy tissue in the uterus. The pills are known for feeling unpleasant, causing intense cramping and bleeding for several hours related to the length of the pregnancy. Pill abortions range from 94% to 98% effective at terminating pregnancy, but require a health center’s approval for the prescription. The effectiveness of the pill decreases the further along a pregnancy is unless an extra dosage is prescribed. Unlike emergency contraception, there are no over-the-counter options for abortion.
Suction abortion or vacuum aspiration is the most common in-clinic abortion procedure with a 99% effectiveness rate. It’s performed on pregnancies between 14 to 16 weeks along and gently sucks the embryo/fetus from the body.
Pregnancies at 16 weeks or more must be terminated by dilation and evacuation, which uses a combination of suction and medical tools to remove the fetus. It also maintains a 99% efficiency rate like vacuum aspiration.
All-Options is a toll-free talkline that can be reached at 888-493-0092, giving professional emotional support and resources on pregnancy, adoption, parenting, infertility, and abortion in a non-judgmental space and is more advisable than traditional “abortion hotlines,” which use misinformation to scare callers.
Most abortions occur in an abortion clinic or hospital, although they can be performed in a variety of settings. Planned Parenthood is most known for abortion services, but they’re also the leading provider of all reproductive healthcare services in the United States.
AbortionFinder is the best way to find a provider near you, which uses information based on your location, age, and pregnancy state to recommend nearby legitimate clinics.When seeking information about abortion, it’s important to look out forcrisis pregnancy centers (CPCs) or “fake clinics.”
CPCs and mobile vans look exactly like real health centers but are run by anti-abortion activists to promote their agenda and scare, shame, and pressure individuals into continuing their pregnancies. After promising to provide pregnancy testing, counseling, and STD testing, they use false information to miseducate people about abortions, birth control, and sexual health – and they do everything in their power to look legitimate by using biased doctors, providers, and researchers (who have been kicked out of the larger legitimate scientific community). Since CPCs are not real clinics, they are not required to adhere to any of the laws real clinics have to – like HIPAA. It’s not uncommon for CPCs to share personal and private information with other organizations and CPCs to continuously harass you.
These numbers indicate that despite the false rhetoric by anti-abortion activists, third-trimester abortions are extremely rare. Most often, these late-term abortions happen because of health concerns or other causes unrelated to simply “not wanting” a pregnancy. By the third trimester, the majority of pregnant individuals have already had their baby shower, have told their friends and family members of their upcoming birth, and very likely have names picked out. All abortions are necessary since first-trimester abortions prevent unwanted pregnancies that are at a higher risk of poverty, illness, and abuse in homes unable to sustain them whereas third-trimester abortions are medically necessary to preserve the life of the would-be mother.
The overturn of Roe v. Wade means that each state is given the complete freedom to determine which abortions are legally allowed to be performed, if any. Before the Supreme Court’s decision, every state had to legally permit abortion in some capacity although they were still given the freedom to regulate abortion past the first trimester.
This has led to some horrific situations that the rest of the world looks down upon – like forced pregnancies by children through rape and incest. There are states with no minimum protections, and political figures that claim to be protecting children from LGBTQIA+ people actively cause them harm – such as the 10-year-old who made national headlines when she had to travel from Ohio to Indiana for an abortion after being raped post-Roe.
There’s a lot of political discourse that could be written here, but the short version is that religious and conservative groups are disproportionally more likely to assault, groom, and generally harm children through abuse, rape, and legislation than queer and transgender people. However, a growing number of conservative-controlled states are entirely banning abortion in all forms and criminalizing the act – as well as calling for a national abortion ban to criminalize abortion outside of their own state jurisdiction.
2 + Abortions is a collection of stories, support groups, and testimonies of individuals who have had two or more abortions in their lifetimes. Their website is geared to dismantled the stigma and shame associated with abortions.;
Abortion Care Network is a national association of independent community-based abortion care providers, which make up the majority of abortion professionals in the United States.
Abortion Diary Podcast is a story-telling platform to share the experiences of the millions of people who have had abortions.
Abortion Finder is a search tool to connect users with over 750 verified abortion providers across the United States, using information like age, location, and last menstrual cycle to list clinics.
Abortion Out Loud is a national network through Advocate for Youth to support young people in need of abortion services or support.
Abortion on Demand provides abortion pills via mail around the US in judications where they are legally allowed to do so through telehealth.
Abortion on Our Own Terms is an advocacy campaign that seeks to change the culture surrounding abortion – especially self-managed abortion done through abortion pills.
Abortion Resolution Workbook is a free resource for individuals wanting self-help with emotional and spiritual conflict after an abortion.
ACLU Reproductive Freedom Project is a litigation and advocacy program of the American Civil Liberties Union to uphold the rights of individuals to freely seek sexual education, contraception, abortion, prenatal care, and childbearing assistance.
Advancing New Standards in Reproductive Health is a research program based at the University of California San Francisco that conducts multidisciplinary research on sexual and reproductive health.
Advocates for Youth is a collective for youth people’s access to reproductive and sexual health, which partners with thousands of youth-focused organizations around the country.
Aid Access facilitates online abortions in all US states with FDA approved abortion pills. The site uses telehealth alongside licensed providers to mail abortion pills to be used at home.
Alliance for Period Supplies hosts a network directory of organizations throughout the United States that provide free period products like pads and tampons.
All-Options, formerly known as Backline, is a toll-free talkline for abortion, pregnancy, parenting, and adoption support available in the United States and Canada.
AMAZE is a free series of sexual health videos hosted on YouTube that uses animation to education young people, parents, and teachers with age-appropriate content.
American College of Obstetricians and Gynecologists is a professional association of providers that are specialized in obstetrics and gynecology to ensure best medically accurate and up-to-date practices in the field.
American Sexual Health Association operates Yes Means Test, a free tool that allows users to find free and confidential STD testing throughout the country based on their zip code and CDC information.
Apiary for Practical Support is an online directory of organizations across the US that provide logistical assistance for people seeking abortion, referred to as Practical Support Organizations (PSOs).
Bedsider is an online birth control support network for individuals between the ages of 18 to 29 through Power to Decide, which explains various birth control methods with comprehensive information.;
Centers for Disease Control and Prevention (CDC) is the official national public health agency of the United States that operates under the Department of Health and Human Services to control, prevent, and treat disease, injuries, and disability in the general public. The CDC is staffed by the current presidential administration to tackle ongoing health concerns and educate the American public.
Center for Excellence in Transgender Health advances health equity and research among transgender and nonbinary communities through the University of California San Francisco.
Center for Reproductive Rights is a global human rights organization that uses partnered attorneys and advocates to ensure reproductive rights are protected in law. Their websites maintains comprehensive information about reproductive health and abortion laws to help users visualize data.
Condom Collective is an Advocates for Youth program made up of youth-led grassroots movements to normalize condom use on college campuses by distributing free condoms and sexual health information.
Doctors Without Borders is an international non-governmental organization that provides free medical and mental health care to people in need, including abortion services in crisis communities they serve.
Ending a Wanted Pregnancy is a group for individuals who made the decision to end a wanted pregnancy, often due to a poor prenatal diagnosis or maternal health reasons.;
Exhale Pro-Voice is a confidential textline available in the United States and Canada for post-abortion emotional support. While Exhale Pro-Voice does not sell abortion pills, they provide professional counseling support.
Fòs Feminista is an alliance of over 250 organizations around the globe that work to advance sexual and reproductive health, rights, and justice.
Guttmacher Institute is a leading research and policy organization that provides data on reproductive topics like abortions, contraception, and STDs.
How to Use Abortion Pill is an online community that shares facts and resources on the abortion pill, such as how to access and use the pill and what to to expect while having a pill-based abortion.
If/When/How is an association and movement for lawyers dedicated for reproductive justice, which also provides funding for bail and legal fees associated abortion, pregnancy issues, immigration, and criminal law.
I Need An A uses non-personally-identifiable information to connect users temporarily with abortion providers most relevant for their circumstance, which is deleted and not stored afterwards. I Need An A works with organizations like Abortion Care Network, Apiary for Practical Support, and the National Network of Abortion Funds to be a starting point for individuals unsure where to begin regarding abortion care.
Ipas is an international non-governmental organization that improves access to abortion and contraception around the world, especially in Africa, Asia, and Latin America.
Ipis Reproductive Health conducts research to advance sexual and reproductive health rights around the world, such as in the United States, Latin America, Caribbean, and Africa.
Just the Pill is a mobile telehealth clinic that mails abortion pills, contraception, and other sexual health services to users in select US states.;=
Love is Respect is a project of the National Domestic Violence Hotline that serves as the national resource in the United States regarding domestic violence for young people ages 26 and younger.
Marie Stopes International, also known as MSI Reproductive Choices, works in 36 countries to provide reproductive healthcare such as birth control and abortion.
Miscarriage + Abortion Hotline is a free hotline for people seeking information and support on abortion and miscarriages through experienced healthcare professionals.
Out2Enrollconnects LGBTQIA+ people and their families with any and all healthcare coverage options through the Affordable Care Act, including Medicaid, Medicare, and commercial insurance. O2E helps users compare plans based on LGBTQIA+ factors, like gender-affirming care or coverage for same-sex partners.
Our Bodies Ourselves is a comprehensive website that provides information on sexual health topics, including abortion, birth control, menstrual cycles, menopause, pregnancy, and more. The site also writes related news articles and posts about topical sexual health information and events.
National Abortion Federation is a professional association of abortion providers, which includes private and public providers. NAF also hosts the National Abortion Hotline – the largest toll-free multi-lingual hotline for abortion information in the US and Canada.
National Network of Abortion Funds is a directory of organizations that provide financial assistance for individuals seeking abortion care. There is a large number of financial providers across the United States, but they operate in small localized regions – so NNAF connects users to relevant organizations they are eligible for.
Pills by Post is a trusted online abortion pill provider that uses telehealth to prescribe abortion services in select approved states. While they operate in less state than other online abortion providers, Pills by Post is significantly cheaper if paying for services out of pocket.
Plan C Pills connects users with online abortion providers in all US states, although they do not directly provide abortion pills themselves. Plan C Pills provides abortion advice and options for all users, even in states where abortion is completely banned and criminalized.
Planned Parenthood is the largest reproductive health services provider in the United States. Although not an FQHC, Planned Parenthood has several safety nets in place to see patients regardless of their ability to pay. In addition to screenings, gender-affirming care, and abortion services, Planned Parenthood also provides free condoms, emergency contraception, and sexual education – including trained counselors available via online chat.
Power to Decide operates a number of other important resources included in this list, like AbortionFinder and Bedsider, as well as other initiatives aimed to advance reproductive health in the United States.
Reddit is a social media platform that operates through thousands of forums (referred to as subreddits) for users to find related communities and discussions. Relevant subreddits include: r/abortion, r/STD, r/auntienetwork, r/antinatalism2, r/prochoice, r/pregnant, r/Miscarriage, r/birthcontrol.
ReproCare is an anonymous healthline that provides accurate information and emotional support about reproductive and sexual health.
Reproductive Freedom for All mobilizes activists and allies to fight for better access to abortion, birth control, paid parental leave, and protections from pregnancy discrimination.;
Reproductive Health Access Project trains and supports healthcare providers to create health equity within the sexual wellness and reproductive healthcare field.
Repro Legal Helpline provides free legal advice about abortion, pregnancy loss, and birth. In addition to their telephone services, their website also provides guidance on abortion laws and policies, as well as associated protections and criminalization.
Resources for Abortion Delivery gives grant funding, technical assistance, and legal compliance assistance to abortion providers in the United States.;
Safe2Choose is an online community that supports individuals seeking abortion with counseling and information with pro-choice healthcare providers.
Safe Abortion Access Fund is a global fund that provides financial support to low and middle income countries around the world in need of abortion advocacy, research, and attitude-transformation.
Scarleteen is a massive online resource and advice website for comprehensive LGBTQIA+-inclusive sexual and relationship education. They have been operating their message boards, advice columns, live chat, and text service for decades.;
Self-Managed Abortion Safe and Supported is a project of Women Help Women to support the rights of people seeking information and access to abortion in the United States.
Sex, Etc. improves teen sexual health through free education resources, videos (like AMAZE), glossaries, and advice to connect young people with accurate data on sex, relationships, pregnancy, STDs, birth control, sexuality, gender identity, etc. It’s operated by Answer, a national organization that promotes sexual education for all ages.
SisterSong Women of Color Reproductive Justice Collective is a national membership organization for individuals and organizations centered on improving reproductive policies that impact marginalized communities – such as women of color.
United Nations Population Fund is the official agency under the United Nations that manages sexual and reproductive health programs to promote gender equality and safe access to reproductive services.
We Testify is a platform for individuals who have had abortions to tell their stories and experiences, creating better representation and visibility of abortions and those who receive them.
Who Not When is a people-centered resource for information and support on late-term abortions, and how abortion bans negatively impact reproductive health.
Women on Web is an international nonprofit that works to provide safe abortion pills in 200 countries via their online consultation.
Women’s Reproductive Rights Assistance Project is the largest independent nonprofit abortion in the United States, which provides financial assistance for abortion care and emergency contraception.
World Health Organization is the international authority on health research and best practices, which asserts that access to all healthcare (including sexual and reproductive healthcare) is a fundamental human right alongside the United Nations.
Young Women of Color 4 Reproductive Justice Collective is an Advocates for Youth program for women of color between the ages of 14 to 24, which aims to dismantle the discrimination and stigma young women of color experience while pursuing abortions.
Youth.GOV Adolescent Sexual Health is a government website that strengthens youth programs in the United States, which includes sexual health.
Understanding the U.S. Healthcare System for Transgender Patients
Transgender people are individuals, so access to the entire healthcare system is important to support holistic health. Although not all medical providers offer gender-affirming treatments, many of them still support transgender lives.
The human body is complex. Healthcare professionals dedicate years to learning a field to provide the best possible care to patients. The basic types of healthcare professionals in the United States are:
Primary care providers
Urgent care
Emergency care
Walk-in care
Telehealth care
Specialist care
Primary Care Providers (PCPs): Your First Point of Contact
Primary care providers (PCPs) are the healthcare professionals you see most often, often referred to as a general or family doctor. PCPs serve as the first point of contact for most needs and are employed at community health clinics, offices, and hospitals.
PCPs address basic health concerns and work to ensure access to continuous care in their communities. Primary providers manage the public via preventive care. This includes vaccinations, wellness checkups, routine screenings, PrEP, birth control, and more. Preventive services must be covered for free or low-cost by all healthcare coverage providers. However, services can only be covered when performed by an approved PCP.
When primary care providers are not equipped to handle a health concern, they refer individuals to specialist providers. In most cases, you must see a PCP FIRST. The primary provider’s office will set up the referring appointment for you. Specialist providers work from private practices, clinics, and hospitals to see patients as needed.
Medical Specialists and the Referral System
Specialists are medical professionals with expertise in fields like allergies and pregnancy. Individuals see specialists when needs cannot be met with primary providers. Specialists do not see patients for basic needs.
In the United States, individuals typically need to be referred by a PCP before they can see a specialist – although there are exceptions, like gynecology. This referral system exists to ensure patients see the correct specialist for their condition AND to make sure treatment will be covered by insurance.
Gender-affirming care, such as hormone replacement therapy and surgery, is provided by specialists. Some primary care providers offer HRT, but most transgender individuals see endocrinologists for hormones like testosterone and estrogen. Surgery is completed by urologists, gynecologists, urogynecologists, plastic reconstructive surgeons, and similar specialists.
Walk-In Clinics: Minor Illnesses and Misconceptions
Walk-in clinics provide low-cost healthcare at retail stores, supermarkets, and pharmacies, bypassing the need to visit a doctor’s office. Also known as retail clinics, convenient care clinics, and nurse-in-a-box, these are operated by a physican assistant or nurse practitioner without full doctor supervision to offer basic care for minor illnesses and preventive services.
Since walk-in clinics operate out of convenience, they are rarely free or covered by insurance. Common walk-in clinics in the United States include CVS, Walgreens, Walmart, and Kroger. When community health clinics and hospitals are not available, retail clinics are a great way to manage minor illnesses and injuries.
There are pervasive misconceptions that some walk-in clinics offer gender-affirming care. This is wholly untrue. Although there are informed consent clinics that provide gender-affirming care to patients without lengthy letter requirements, these are operated by licensed doctors who evaluate patients before prescribing treatment like hormone replacement therapy.
Telehealth Services and Online Gender-Affirming Care
Telehealth services are provided by a medical professional from a remote location. These services are conducted over video call, phone call, or remote monitoring to allow individuals to access care without driving to a local clinic.
Most providers offer telehealth options, whether it’s electronic messaging through patient portals or full digital appointments. However, not all providers and conditions are eligible for telehealth. Although telehealth is a great substitute for primary and specialist care, certain services like vaccinations and laboratory exams require in-person visits.
Many transgender individuals access hormone replacement therapy through telehealth. Telehealth HRT providers (ex. Plume, FOLX, QueerDoc) may only prescribe treatment in states where they hold active licenses. HRT is legally accessible via telehealth throughout the entire United States, although some providers may not serve all states and territories.
In 2023, the DEA implemented new federal laws creating barriers to testosterone via telehealth. Although feminizing HRT can be prescribed entirely through telehealth, the DEA seeks to require individuals to be seen in person to be prescribed testosterone. However, the DEA has continued to extend COVID telemedicine guidelines to allow testosterone prescription until December 31, 2026.
Urgent Care Clinics: Bridging the Gap in Medical Care
Urgent care clinics are walk-in facilities that treat non-life-threatening conditions requiring prompt treatment. These clinics do not need appointments to see patients and bridge the service gap between generic primary care and the emergency room.
These facilities are best for illnesses and injuries that cannot wait for a doctor’s appointment, but do not require critical care from an emergency room. Urgent care clinics commonly see sprains, burns, and flus.
Urgent care clinics are not always available, especially in rural communities. In areas without urgent care facilities or retail clinics, primary care providers at community health clinics often offer same-day walk-in services.
Emergency Services: Critical Care and Triage Hierarchy
Emergency services provide immediate medical treatment to prevent serious harm or death. Unlike urgent and primary care, emergency providers treat sudden, severe, and life-threatening conditions. Emergency facilities are staffed 24/7 with trained physicians, nurses, and specialists to treat intense situations.
To best serve public health, individuals are directed to facilities based on their needs. Most situations only require basic intervention and are thus best served by primary providers and walk-in clinics to avoid overwhelming urgent and emergency services. The implementation of urgent care facilities directs non-critical patients out of the emergency room for treatment.
In the United States, emergency services are expensive. Most treatment performed inside US hospitals is exponentially more expensive than treatment provided at community health clinics or urgent care facilities.
Navigating U.S. Healthcare Coverage and Insurance Systems
Understanding healthcare coverage is fundamental to accessing medical treatment.
In the United States, healthcare professionals cannot refuse patients experiencing life-threatening conditions, BUT patients can be billed incredibly large amounts of debt for treatment provided. Treatment and billing can occur even if you are unable to consent before treatment.
There are four types of healthcare coverage. The United States uses all four coverage systems in some capacity.
What is Universal Healthcare: Single-Payer Systems
Universal healthcare refers to coverage systems that provide medical treatment to all people, regardless of their ability to pay. Universal healthcare is also called single-payer because all medical treatment is paid for by a single entity: the government.
Medical treatment is never free because facilities must be continuously maintained. Universal healthcare systems work by using taxpayer funds to offset the cost of medical services.
The Beveridge Model: Socialized Healthcare and U.S. Applications
Beveridge healthcare systems provide medical treatment almost entirely through government funds. In countries with predominantly Beveridge systems, most medical facilities are operated by the government. These systems are classified as socialized, providing treatment to everyone regardless of income.
The Beveridge system was coined by Sir William Beveridge and Nye Bevan, creating the National Health Service (NHS) in the United Kingdom. Bevan successfully campaigned against Winston Churchill by promising the British public reformed welfare services. Through taxpayer funds, Bevan and Beveridge successfully created a system to provide British citizens with better medical treatment.
Societies that have normalized socialized healthcare, like the United Kingdom, view healthcare as a responsibility of the government. As the government is obligated to take care of its citizens by funding roads and schools, these publics believe healthcare is an obligation they are jointly entitled to. After normalization, governments cannot defund socialized healthcare without massive public backlash because it benefits the entire society.
The Beveridge socialized model is used in the United Kingdom, Spain, Cuba, New Zealand, and many other countries. Further, the government’s involvement forces commercial healthcare providers to keep costs low to compete with free government services.
The Beveridge model is used to maintain the Department of Veterans Affairs, Indian Health Service, and Federal Bureau of Prisons. The United States employs the Beveridge model in select contexts, although many politicians like Bernie Sanders and AOC advocate for greater usage. Individuals using these systems visit government-operated facilities to obtain free medical treatment covered by taxpayer funds.
These systems do not eliminate free market competition. Even in countries that rely entirely on Beveridge socialized healthcare, individuals reserve the right to obtain professional care outside of the government system. For example, British citizens can find licensed providers outside of the NHS, and veterans may obtain care outside of Veterans Affairs. Although they must pay out-of-pocket or use alternative coverage for these providers, they receive care much faster than generic socialized treatment.
What is Privatized Healthcare: Market-Based Systems
Privatized healthcare refers to coverage systems that rely on individuals’ ability to pay for medical treatment. Access to treatment depends entirely on one’s ability to pay for services.
United States law prevents medical professionals from refusing life-threatening treatment, even if an individual cannot pay. However, unpaid treatment is billed and owed to patients (even if they cannot consciously consent to treatment).
The Bismarck Model: Private Insurance and Employer-Sponsored Care
Bismarck healthcare systems provide medical treatment through private insurance companies that reimburse medical facilities for services. Bismarck models are classified as privatized healthcare because access to treatment is based on one’s individual ability to pay.
Most often, insurance companies are paid through mandatory payroll deductions by employers to provide coverage to employees. The system was originally coined by Otto von Bismarck, who needed to create a new system in the wake of economic crisis in the German Empire.
Approximately 60% of all Americans maintain treatment coverage from private insurance companies through an employer. When Americans make too much income to qualify for other coverage options, they must utilize private insurance or pay for medical treatment entirely out-of-pocket. Private insurance can be offered through employer payroll deductions or bought privately. Marketplace subsidies exist to offset costs with non-employer private insurance.
Most Americans are deeply unsatisfied with privatized healthcare, leading to the complex public reaction regarding United States v. Luigi Nicholas Mangione. Although other countries apply legislation to regulate the cost of private treatment, the United States does not set any limits to deter massive medical debt or ineffective private coverage.
Understanding National Health Insurance: Medicare, Medicaid, and Single-Payer Delivery
Countries do not have to fully implement Beveridge’s socialized or Bismarck’s privatized systems. Dozens of countries implement models that combine these overarching systems to create National Health Insurance (NHI).
In NHI systems, the government operates as a single-payer entity to fund medical treatment through taxpayer funds. Unlike socialized medicine, the government does NOT own healthcare facilities; hospitals, clinics, and providers are private businesses that accept National Health Insurance as a payment coverage.
Similar to socialized medicine, NHI systems do not negate commercialism. NHI systems allow individuals to hold secondary private coverage to obtain care outside the primary referral system – NHI simply ensures all citizens have basic coverage.
Countries that predominantly use the NHI system include Canada, South Korea, Australia, and Italy. The United States employs NHI via Medicaid and Medicare, operating as a single-payer agency to cover medical treatment provided by private healthcare facilities.
The Major U.S. Healthcare Programs and Insurance Options
The United States uses all four coverage types to provide healthcare to citizens. Understanding your coverage eligibility connects you with treatment options without paying out-of-pocket.
Healthcare is disproportionately more expensive in the United States than elsewhere. The United States continues to be the only high-income country in the world that does not guarantee basic medical coverage (universal healthcare) to all its citizens. This results in the majority of Americans relying on commercial insurance companies for treatment.
Commercial healthcare coverage does not equate to better treatment or fewer medical bills.
Insurance companies create complicated contracts to avoid paying for treatment, forcing patients to pay deductibles in addition to insurance subscription fees.
Insurance companies are well-known for denying medically necessary care. Insurance executives determine coverage eligibility without medical education, determining profits over prescribed treatments.
Individuals can be covered by more than one coverage policy. In other words, having commercial insurance does not prevent you from obtaining Medicaid, veterans’ benefits, etc.
Medicaid: State-by-State Eligibility and Low-Income Coverage
Medicaid is a joint federal and state program that provides free health insurance (NHI) to certain populations. Eligibility is determined individually by states and territories, although common covered populations include:
Low-income individuals
Pregnant individuals
Children
Elderly individuals
Individuals with disabilities
Florida, Alabama, and Tennessee have some of the strictest Medicaid eligibility requirements. In states like these, you must be actively parenting a dependent child, pregnant, Disabled, or older than 65 years old. Further, legally able-bodied adults with children are ONLY eligible if they make 18% or less than the federal poverty line ($235 per month in 2026).
California, New York, and Massachusetts have the greatest Medicaid eligibility. In addition to generic populations like above, these states provide Medicaid to all single adults who make up to 138% of the federal poverty line ($1,835 per month in 2026).
Income eligibility increases with household size. Currently, nine states do not allow childless adults Medicaid coverage regardless of income. Some states provide Medicaid coverage to non-citizens, although immigrant eligibility varies. Use the Medicaid and CHIP Scorecard to review local policies.
Does Medicaid Cover Gender-Affirming Care?
Yes, Medicaid can cover gender-affirming care, but coverage depends on state residency. Medicaid eligibility and guidelines are determined by states. Over half of all US states, DC, and Puerto Rico explicitly cover gender-affirming care in Medicaid. On the other hand, one quarter of states explicitly forbid Medicaid from covering gender-affirming care.
Executive Order 14187 forbids all Medicaid and CHIP coverage from covering any gender-affirming care for individuals under the age of 19. Order 14187 was blocked through a federal injunction in PFLAG v. Trump and Washington v. Trump. Due to the injunction, minors may receive Medicaid and CHIP coverage for gender-affirming care based on state guidelines.
CHIP: Expanding Healthcare Coverage for Low and Middle-Class Youth
Individuals up to age 19 are eligible for the Children’s Health Insurance Program, even if their household income is too high for Medicaid requirements. The income threshold for CHIP ranges from 200% to 300% of the federal poverty line, depending on state regulations.
CHIP was created to ensure American youth maintain coverage through a national health insurance. Although Medicaid provides coverage to low-income individuals, the middle class is left without healthcare coverage if their income is too high for Medicaid but not enough for commercial insurance.
Like Medicaid, states are given the authority to determine eligibility requirements. States like North Dakota limit coverage to youth up to 175% of the federal poverty line, while New York covers up to 405%.
Unlike commercial health coverage, which is required to cover youth under their parent’s plan until age 26, young people lose CHIP upon turning 19. On their nineteenth birthday, former CHIP youth become uninsured unless they obtain alternative coverage.
Yes, CHIP can cover gender-affirming care, but coverage depends on state residency. CHIP eligibility and guidelines are determined by states. One quarter of all US states explicitly forbid CHIP from covering gender-affirming care. In addition, half of the United States bans all gender-affirming care for minors – regardless of whether it is through CHIP, commercial insurance, or out-of-pocket.
Executive Order 14187 forbids all Medicaid and CHIP coverage from covering any gender-affirming care for individuals under the age of 19. Order 14187 was blocked through a federal injunction in PFLAG v. Trump and Washington v. Trump. Due to the injunction, minors may receive Medicaid and CHIP coverage for gender-affirming care based on state guidelines.
Medicare: Federal Coverage for Seniors and Individuals with Disabilities
Medicare is a national health insurance for individuals with disabilities OR aged 65 and older. Unlike Medicaid, Medicare does not have any income eligibility limitations, although Medicare generally reduces healthcare costs rather than fully covering them, as Medicaid does.
People can be covered simultaneously by Medicare and Medicaid if they meet eligibility requirements in their state, heavily assisting low-income seniors and people with disabilities.
Medicare reduces out-of-pocket expenses associated with hospital care, outpatient services, prescription medication, and private healthcare plans. Since Medicare is operated solely as a federal program, it has no state flexibility.
Does Medicare Cover Gender-Affirming Care?
Yes, Medicare covers gender-affirming care when deemed medically necessary. Since Medicare is operated federally, this coverage extends to all states and territories.
The Trump-Vance administration seeks to eliminate gender-affirming care, although they have had limited success. Despite the block of Order 14187, the Trump-Vance Centers for Medicare & Medicaid Services are still trying to remove access. Currently, gender-affirming care through Medicare is protected, although the CMS states coverage is determined on a case-by-case basis.
VA Healthcare and TRICARE: Medical Coverage for Military Families
Individuals who have served in the United States armed forces AND have never received a dishonorable discharge are eligible for complete healthcare coverage. As a Beveridge-style system, veterans may receive free medical treatment at any VA facility.
Current service members have medical services covered through TRICARE, a program run by the United States Department of Defense. After serving for at least 24 continuous months in the military, service members become eligible for honorable discharge benefits, including VA healthcare. Immediate family members of service members and veterans are automatically eligible for coverage.
There are no income restrictions for VA healthcare coverage. For medical treatment to be covered for free, individuals generally must receive care at VA facilities. However, VA healthcare has notoriously long wait times for treatment, which is why covered individuals may elect to see other providers with alternative coverage or out-of-pocket.
Does VA Health Insurance Cover Gender-Affirming Care?
No, the Department of Veterans Affairs currently does not provide coverage for gender-affirming care due to the Trump-Vance administration’s Order 14183. This restriction applies both to active servicemembers and veterans.
The Indian Health Service (IHS): Tribal Eligibility and Federal Care
Native Americans are eligible for complete healthcare coverage through the Indian Health Service. As a Beveridge-style system, individuals may only receive free medical treatment through IHS facilities.
To be eligible for IHS services, individuals must be affiliated with a federally recognized tribe. Similar to VA healthcare and TRICARE, individuals may elect to see providers outside of the IHS system through alternative coverage or out-of-pocket. Also, like VA healthcare and TRICARE, IHS coverage does not have any income restrictions.
Yes, the IHS covers gender-affirming care. Federal policy states that individuals under IHS coverage are entitled to gender-affirming coverage. Additionally, since IHS clinics operate with sovereign immunity, they may provide gender-affirming care despite restrictive state laws.
Specific coverage depends on your local IHS, Tribal, or Urban Indian clinic. If an IHS facility cannot provide gender-affirming services directly, IHS may cover the cost to see an outside provider through the PRC program.
Incarcerated Healthcare: Constitutional Rights and Carceral Systems
Incarcerated individuals maintain a protected right to medical treatment while in government custody. As a Beveridge-style system, individuals receive reduced medical treatment from approved government providers.
Individuals who are currently serving in United States prisons or jails are restricted from traditional healthcare coverage options, including the Marketplace.
However, the quality of medical service provided to incarcerated individuals varies drastically because there are no federal standards. While Estelle v. Gamble established that inmates are entitled to healthcare, there is no consensus on what minimum treatment must be provided for free.
Many facilities, even those accredited by the National Commission on Correctional Health Care and American Correctional Association, enforce mandatory copays on inmates. These copays are disproportional to inmate income; on average, inmates earn $0.25 to $0.86 per day, although it costs $13 for a single sick visit.
Federal law only stipulates that prisons and jails must provide medical treatment and does not define the cost or quality of care provided. These conditions deter most inmates from seeking medical care.
Do Prison Providers Cover Gender-Affirming Care?
Yes, prison providers may provide gender-affirming care, but it is extremely difficult to acquire. Treatment also depends on whether you are residing in a state or federal facility. Denial of gender-affirming care is classified as cruel and unusual punishment.
In federal facilities, inmates have a protected right to gender-affirming care. Executive Order 14168 abolished existing transgender care guidelines and attempted to ban gender-affirming care at all federal prisons. Although the Transgender Offender Manual no longer applies, federal courts have blocked the ban on gender-affirming care.
In state facilities, gender-affirming care is determined by the states. Some states offer complete coverage for gender-affirming treatment, while others bar access entirely to forcibly detransition inmates. Most states use “freeze-frame” policies that allow inmates to continue prescribed gender-affirming care upon incarceration.
The Health Insurance Marketplace and Employer-Sponsored Plans
Most Americans obtain commercial healthcare coverage through the Healthcare Insurance Marketplace if they do not qualify for alternative coverage like Medicaid, IHS, or VA. The Marketplace is a Bismarck-style system since medical treatment is paid through private companies that reimburse providers for services.
The Marketplace originated from the 2010 Affordable Care Act (Obamacare). When employers do not offer sufficient insurance coverage, individuals use the Marketplace to choose coverage or confirm eligibility for government options like Medicaid. As private coverage providers, Marketplace options offer individualized contracts with deductibles, copays, and limitations.
Based on demographics and income status, the Marketplace will display all available coverage options. All individuals are eligible for commercial Marketplace insurance as long as they are at least 18 years old, are living legally in the United States, are not eligible for Medicare, and are not currently incarcerated.
Most United States employers are required to offer healthcare insurance options to employees. These are private plans similar to options available on the Marketplace. Only small employers with 50 or fewer full-time employees may opt out of providing insurance options to staff under the Affordable Care Act.
Do Marketplace and Commercial Plans Cover Gender-Affirming Care?
Yes, Marketplace and commercial insurance can cover gender-affirming care, but it depends on state residency. Approximately half of all US states explicitly prohibit private insurance providers from not covering gender-affirming care. Only two states (Arkansas and Mississippi) allow private companies to refuse gender-affirming coverage.
The Trump-Vance administration has removed gender-affirming care’s status as an “Essential Health Benefit” for Marketplace providers, although this will likely have little impact. Even in states that do not explicitly require private insurance companies to cover gender-affirming care, private insurance cannot discriminate against sex assigned at birth under the Affordable Care Act. The ACA does not allow blanket bans on medically necessary treatments, which include blanket bans on gender-affirming care.
Overcoming Cost Barriers: Free and Low-Cost Healthcare Options
Cost is the leading barrier that prevents Americans from accessing medical treatment. When individuals avoid preventive healthcare, they become at risk of life-threatening emergencies. These are programs and initiatives that make healthcare accessible.
Understanding FQHCs: Affordable Treatment and Community Clinics
Federally Qualified Health Centers (FQHCs) are federally funded nonprofit health organizations that provide medical treatment on a sliding scale. Through government funding, these organizations can offer services regardless of individuals’ ability to pay.
FQHCs often host public events for their communities to provide limited preventive care for free, like annual check-ups, immunizations, and screenings. Additionally, FQHCs always accept government healthcare coverage options like Medicaid, CHIP, and Medicare.
FQHC and similar healthcare organizations provide non-emergency medical transportation (NEMT) to provide transportation to appointments. Transportation is provided for free or at a discounted rate based on income status. Some NEMT is operated through agencies like Uber Health and Transdev.
Some Federally Qualified Health Centers may offer gender-affirming care, but this depends on whether they have providers trained in services such as hormone replacement therapy. The endocrinologist who has prescribed my HRT for the last eight years is through a FQHC.
You should always be treated with dignity, regardless of gender identity, although discrimination laws vary from state to state.
Charitable Healthcare Facilities: Free Medical Treatment for the Uninsured
The NAFC maintains a list of clinics that provide free or reduced services. There are over 1,400 clinics currently affiliated with the NAFC that provide treatment for free, even if you do not have insurance or coverage. Similar programs exist for pharmacy medications, vision care, and dental health.
These nonprofit facilities operate through volunteers, donations, and grant funding that allow them to serve uninsured or underinsured communities.
Like FQHCs, charitable healthcare facilities can potentially offer gender-affirming care – although it is unlikely since most clinics are gears towards preventative and emergency health. The largest charity-like HRT provider is Planned Parenthood, which offers gender-affirming care on a reduced sliding scale based on need.
Direct Primary Care (DPC): Subscription-Based Medicine Without Insurance
Direct Primary Care (DPC) requires patients to pay monthly membership fees to a healthcare facility directly for ongoing access to care, rather than involving any insurance company. It is a model of healthcare coverage recently introduced to the United States.
Instead of insurance deducting from each paycheck, DPC is essentially a subscription to your local clinic. In exchange for membership, patients gain access to unlimited primary care visits, lab work, and other services without copays or deductibles. However, these facilities do not accept commercial insurance, Medicaid, CHIP, Medicare, or other forms of coverage.
There are several websites that maintain directories of DPC facilities throughout the United States, such as DPC Alliance.
Although possible, it is extremely unlikely for any DPC to provide gender-affirming care. Since these facilities cater to primary care needs, they are unable to fulfill specialist requests like hormone replacement therapy.
GoodRx is a website and mobile application that links users with discounts for prescription medication. Its coupons can be used at over 75,000 pharmacies across the United States, including major retailers like Walmart, CVS, Costco, and Kroger.
GoodRx is also a price comparison tool, allowing users to find the best price for their medication at multiple retailers.
In February 2026, Trump announced the launch of “TrumpRx.” Although TrumpRx is government-funded, it is an inferior knock-off of GoodRx. Based on my limited use of the website, TrumpRx gives worse discounts, focuses on affiliated brands, does not have a comprehensive medication database, and is far too restrictive on who may use these lesser discounts.
The main downside to GoodRx is that you cannot use insurance or other healthcare coverage in combination with its coupons. Although you may use GoodRx while covered by these plans, all medication obtained through GoodRx coupons must be paid out-of-pocket. However, GoodRx’s coupons bring medications down to copay and cost-share fees.
Several programs exist to provide prescription medication through the mail, cutting out the cost of retail pharmacies by shipping medication to consumers from manufacturers. These are the most popular options.
Rx Outreach: Nonprofit Mail-Order Pharmacy Access
Rx Outreach delivers prescription medication via mail, regardless of insurance coverage. It operates similarly to GoodRx to provide deeply reduced medication to underinsured people. Mail delivery is available to anyone in all 50 states, DC, Puerto Rico, and the US Virgin Islands as long as they have a valid prescription for any Rx Outreach medication.
Rx Outreach is especially useful because they have assistance programs to offer free medication to individuals based on federal funding. Although Rx Outreach offers reduced medication to all 50 states, its patient assistance program is currently limited to the St. Louis area.
Although it is available to everyone, Rx Outreach prioritizes individuals who meet specific income thresholds. Similar to GoodRx, Rx Outreach does not accept insurance, and all medication must be paid out-of-pocket.
Amazon Pharmacy: Insurance Integration and RxPass Savings
Amazon Pharmacy provides prescription medication via the mail and, unlike other mail-order pharmacies, accepts most major insurance plans. Amazon Prime Members have access to RxPass, which offers over 60 generic medications for a flat $5 per month subscription fee.
Compared to Rx Outreach and Cost Plus Drugs, Amazon Pharmacy is the fastest, most convenient, and best to use with commercial insurance. However, Amazon Pharmacy is not necessarily the cheapest – many mental health medications are more expensive through Amazon Pharmacy.
Cost Plus Drugs: Opaque Pricing Replaced by Transparent Markups
Cost Plus Drugs sells mail-order medication at a near-wholesale rate, making it useful for individuals with high copays. For each medication, users are charged the manufacturer price, a flat 15% markup, and a $5 pharmacy fee.
Like Rx Outreach, Cost Plus Drugs does not accept insurance. All medication through Cost Plus Drugs must be paid out-of-pocket.
American Academy of Family Physicians. Organization that sets national standards for family medicine and primary care. The AAFP Neighborhood Navigator connects users with over 40,000 social services via zip code, ranging from food, infant supplies, housing, transit, education, employment, etc.
American Academy of HIV Medicine. Organization that provides training, data, and guidance to healthcare professionals regarding HIV care and prevention.
American Public Health Association. National organization of US healthcare providers. Impacts federal legislation and sets national standards for healthcare policies.
CancerCare. Organization that provides free support services and information to the public regarding cancer. Manages support groups, counseling, resource navigation, workshops, publications, and financial assistance.
CaringInfo. Education and resource hub for end-of-life care to provide tools to patients, families, caregivers, and healthcare professionals navigating serious illnesses.
Centers for Disease Control and Prevention. Government agency operated by the United States government to control, prevent, and treat disease, injury, and disability. Since CDC policies and staffing vary based on presidential administration, campaigns fluctuate based on expected health concerns.
CostPlus Drugs. Mail-order pharmacy that reduces consumer fees by cutting out retailers. Users are charged slightly more than manufacturing costs for medication.
Department of Health and Human Services. Government agency that administers over 100 different programs to enhance public health through healthcare coverage, social services, research, and emergency response planning.
Drugs.com. Pharmaceutical encyclopedia that provides information on medication, side effects, and interactions. Also functions as a pill identifier and phonetic search engine, making it the most popular and up-to-date website for medication information.
FOLX. Gender-affirming care telehealth provider. Offers services in all 50 states, although gender-affirming treatments like HRT are only available based on state law. Also provides mental health services, primary care, reproductive services, and fertility treatments.
FQHC Directory. Government directory of health organizations that provide medical treatment on sliding scales. All organizations listed as FQHCs must accept Medicaid, Medicare, and CHIP and provide non-emergency medical transportation upon request.
FreeDentalCare. Directory of free and reduced dental clinics for low-income individuals throughout the United States.
Get Covered Connector. Connects users with local nonprofit organizations to access healthcare coverage and complete applications. Provides telephone, virtual, and in-person appointments with providers. Directory includes information regarding whether nonprofit providers are LGBTQIA+-friendly.
GLMA Health Professionals. Association of LGBTQIA+ healthcare professionals with free educational material and training for medical providers. Maintains online directory of queer-friendly providers at the LGBTQ+ Healthcare Directory.
GoodRx. Website and mobile app that provides discounts for prescription medication at select pharmacies, including major retailers like Walmart, CVS, Costco, and Kroger.
Greater Than AIDS. Provides up-to-date information about HIV and STDs to underserved populations, as well as testing and prevention tools.
Healthcare Insurance Marketplace. Government platform that enrolls users in commercial insurance plans, Medicaid, Medicare, CHIP, and other coverage options.
Healthy Start. Government program focused on maternal and child health and connects new mothers with services, such as transportation, education, and housing assistance.
Human Rights Campaign. Organization centered around LGBTQIA+ advocacy in the United States and maintains many resources related to transgender health, including topics like the Affordable Care Act, healthcare rights, and discrimination reporting. The Healthcare Equality Index annually ranks healthcare facilities regarding LGBTQIA+-inclusive policies.
Lambda Legal. Civil rights organization that promotes LGBTQIA+ equality through litigation and public policy. Maintains several resource collection centers, including one focused on LGBTQIA+ healthcare.
LGBTQ+ Healthcare Directory. Online directory that connects users with information regarding local LGBTQIA+-friendly healthcare providers.
Mayo Clinic. Medical group that allows users to search for information based on the expertise of over 3,000 physicians, scientists, and researchers to inform people about health.
MedlinePlus. Government service that provides health information and contains over 7 million medical journals, books, studies, reports, and microfilms.
Medscape. Media outlet for healthcare professionals that gives medical news, drug development updates, and clinical trial information.
MyHealthFinder. Government service that offers information on wellness and disease prevention. The site uses basic user information to calculate best practices to stay healthy, including medical screenings and vaccinations.
National Association of Free & Charitable Clinics. Directory of healthcare facilities that provide free or reduced services regardless of insurance status. Data directory also includes information related to pharmacies for free prescription medication.
National Eye Institute. Government program that connects individuals with free and low-cost vision services.
National LGBT Cancer Project. LGBTQIA+ cancer support organization that discusses cancer-related topics, clinical trial information, and resources.
National LGBTQIA+ Health Education Center. Educational and consultation program that gives webinars, learning modules, and publications to healthcare providers to better serve LGBTQIA+ patients.
National Maternal Mental Health Hotline. Confidential government service available 24/7 for new and expecting mothers. The hotline can be reached via telephone call, text message, or instant message at 833-852-6262.
Orphanet. Encyclopedia of rare diseases and conditions. Although less popular than MedlinePlus and Mayo Clinic, Orphanet contains critical data on rare conditions and medications.
Out2Enroll. Connects LGBTQIA+ people with healthcare coverage options through the Affordable Care Act, including Medicaid, Medicare, and commercial insurance. Allows users to compare plans based on gender-affirming care, coverage for same-sex partners, and other aspects relevant to LGBTQIA+ people.
OutCare. Organization that creates comprehensive resources for equitable LGBTQIA+ health. Offers paid research opportunities, peer support, training, and webinars. Maintains the OutList Provider Directory and OutCare Saving Program. Also provides free PrEP and DoxyPEP, as well as community resources.
OutCare Saving Program. Provides discounts for prescription medication at select pharmacies.
Planned Parenthood. Reproductive healthcare provider that offers informed consent gender-affirming care through virtual and local clinics.
Plume. Get hormone therapy, mental health support, and ongoing transgender healthcare from licensed clinicians. Access care online, including prescriptions, letters of support, and everyday care services. Available in most states, although testosterone HRT is more restricted.
Poison Control. Tool that provides users with information about common poisons in over 100 languages. Available mobile app, virtual chat, and telephone hotline. Contact your local poison center at 800-222-1222.
Protect Trans Health. National campaign to improve transgender access to healthcare and coordinates advocacy to defend the legal right to gender-affirming care.
PubMed. Provides free access to over 37 million biomedical publications through the National Library of Medicine.
QueerDoc. Gender-affirming care telehealth provider that prescribes to individuals residing in Alaska, California, Florida, Hawaii, Idaho, Oregon, Montana, Utah, Washington, and Wyoming.
Ryan White HIV/AIDS Program. Government agency for HIV primary care, medication, and support services for low-income individuals living with HIV.
Rx Outreach. Nonprofit mail-order pharmacy that delivers affordable prescription medication regardless of insurance status in all 50 states, DC, Puerto Rico, and the US Virgin Islands. Also operates initiatives like Fill the Gap to provide free medication to eligible participants.
The Cancer Network. Resource site for cancer-related information and tools related to LGBTQIA+ people. Operates multiple peer-support groups and a library on clinical information and screenings.
Transbucket. Forum that connects transgender individuals to gender-affirming surgery results.
Trans Health Project. Program operated by Advocates for Trans Equality to provide guidance to users to best navigate health coverage for comprehensive healthcare. Also has a video series explaining the insurance process for gender-affirming care.
Trans Legal Health Fund. Resource by the Transgender Law Center and If/When/How to financially support transgender people facing investigation, arrest, or prosecution while accessing healthcare. Although there is no longer a direct link to the Trans Legal Health Fund, individuals can request assistance through the Help Desk.
WebMD. Directory of information related to diseases, medications, and symptoms. Also maintains a database of medical providers through WebMD Care.
World Health Organization. International agency that leads public health alongside the United Nations.
World Professional Association for Transgender Health. Leading medical association for international best practices regarding transgender health. Provides professional guidance and educational research for evidence-based medicine to best serve transgender people around the world.
Frequently Asked Questions
Can a clinic or hospital refuse to treat me if I am uninsured?
It depends on what type of treatment you are seeking. Federal law requires medical providers to stabilize anyone experiencing an acute health emergency, regardless of their ability to pay. Healthcare professionals may turn away uninsured individuals for preventative primary care or maintenance treatments.
Federally Qualified Health Clinics and Certified Community Behavioral Health Clinics are national safety nets that are required to provide services on a sliding scale to uninsured individuals. FQHCs and CCBHCs also must link individuals with resources, such as Medicaid, to support their communities.
Why do some HRT medications cost drastically more on certain platforms than others?
Pharmaceutical pricing in the United States is influenced directly by corporations and government regulation. Estradiol tablets are easily accessible because it is a generic prescription that cannot be patented. Testosterone is unavailable from mail-order platforms due to restrictive controlled substance laws, so pharmaceutical companies can charge higher retail prices without competition or government regulation to keep prices stable.
Can I use my health insurance alongside direct-to-consumer coupon tools?
No. You typically must choose to either use healthcare coverage or coupons at checkout since discount apps (ex. GoodRx) and cash-pay pharmacies (ex. Rx Outreach, Cost Plus Drugs) operate independently of insurance networks.
When you use a direct-to-consumer coupon, you are bypassing your insurance plan. All money paid out-of-pocket for these medications does not automatically count towards your annual deductible, although some platforms have partnerships with specific plans.
Do I need health insurance to use the mail-order pharmacies or clinics listed in this guide?
No. You do not need commercial insurance to access care. Platforms like GoodRx, Cost Plus Drugs, and Rx Outreach operate on out-of-pocket models that bypass insurance coverage for medication. Further, all Federally Qualified Health Centers must treat patients regardless of insurance status on adjusted sliding-fee scales.
What is the “informed consent model” for hormone replacement therapy?
The informed consent model allows educated adults to access medical treatment like hormone replacement therapy without a psychiatric diagnosis and a therapist’s letter.
This process was the standard when accessing gender-affirming care throughout the last century, but it gatekept individuals from treatment. Through informed consent, medical providers directly educate patients and determine whether they can consent to treatment. Eligible patients can begin HRT immediately rather than waiting six to twelve months of psychiatric appointments.
Transgender individuals are more likely to experience mental health struggles due to discrimination and a lack of support. No one should struggle alone. This guide shares information regarding transgender mental health.
This guide was built by Benito, a former psychiatric crisis responder (MHP/CHW). While these materials were curated using professional crisis intervention frameworks, they are for educational purposes and do not substitute for personal medical advice.
If you are thinking about harming yourself or others, please get immediate support. Visit our crisis resources or contact the National Suicide Prevention Hotline for telephone, text, and online chat services.
Defining Mental Health: A Trauma-Informed Approach
Individuals are considered mentally healthy if they can:
Cope with life stressors
Visualize and improve talents
Engage with their communities
There is more to being mentally healthy than just not being sick. Most people incorrectly associate health with the ABSENCE of sickness. According to the World Health Organization, “health is the state of complete PHYSICAL, MENTAL, and SOCIAL well-being and NOT merely the absence of disease or infirmity.”
By reframing our perception of health, we are empowered to take care of ourselves now. Health professionals recommend active steps towards healthy living rather than waiting until sickness in a practice called “preventative health.”
Health isn’t just the physical body either. To be healthy, we must take care of several aspects of our lives. It’s difficult to keep friendships if you’re stuck in bed; it’s hard to avoid sickness if your home or job is in a polluted area; and it’s tough managing anxiety if you’re unable to socialize.
Under a trauma-informed framework, health professionals are prompted to consider what life experiences formed one’s health conditions. Historically, doctors centered on diagnoses by essentially asking, “What’s wrong with you?” Reframing the question as “What happened to you?” gives providers a wider view regarding what experiences and traumas shaped their patients, creating better health outcomes.
Here are three examples of how trauma-informed care improves outcomes:
Trauma-Informed Care Example #1
Michael is a homeless man trying to get approved to stay at a local shelter. The staff working on Michael’s paperwork asks a lot of questions that he doesn’t know the answer to. Frustrated, Michael lashes out and yells at the worker.
Response A: The worker is offended and does not understand why the situation escalated so quickly. Since this paperwork is critical to allow Michael to stay in their long-term facilities, they assume Michael is either on drugs or does not want to put in the work required to stay there. They might even assume Michael is ungrateful!
Response B: The worker is offended but understands that many homeless people have had traumatic experiences that make them prone to stress. The lack of stable housing causes anxiety, and homeless individuals are statistically likely to have PTSD and suffer assault in comparison to housed populations. Michael behaved inappropriately, but the staff’s knowledge of trauma-informed care allowed them to recenter the conversation and de-escalate before making assumptions about Michael.
Trauma-Informed Care Example #2
Ruth is a lesbian woman working at a retail store. She is approached by an older customer, who wants to make small talk while they shop. Ruth obliges but becomes tense when the customer begins discussing their day at church. Abruptly, Ruth cuts the conversation off and leaves. The customer is confused and tells a supervisor about the strange interaction.
Response A: The supervisor is annoyed that Ruth left the customer mid-conversation. They assume Ruth has poor customer service skills and purposely failed to help the customer do their shopping. The supervisor might even assume that Ruth was judgmental and acted out because she disapproved of the customer’s faith.
Response B: The supervisor is annoyed that Ruth failed to help the customer, but they know that many LGBTQIA+ people have had traumatic experiences related to religion. Since Ruth is a lesbian, religious discussions may cause her stress or anxiety, even if the conversation would have been light-hearted. Ruth reacted inappropriately, but her supervisor’s knowledge of trauma-informed care allowed them to recenter their thinking before making assumptions about Ruth.
Trauma-Informed Care Example #3
Julius is a Black man who is stopped by a police officer while walking home from work. The officer asks him a lot of questions, making Julius increasingly anxious as he tries to get home to his daughters.
Response A: The officer sees Julius’ growing anxiety and assumes that he is hiding something. Julius does not answer their questions fully, wrings his hands, and does not make eye contact with the officer. The officer is suspicious and assumes that Julius is likely committing criminal activity.
Response B: The officer sees Julius’ growing anxiety but understands that many Black Americans have had traumatic experiences with law enforcement. Since Julius is Black, interactions with police officers may make him prone to stress and anxiety, even if he has not committed any crime. The officer’s understanding of trauma-informed care allowed them to reframe how they saw Julius, de-escalating the conversation before jumping to assumptions.
Mental health is affected by trauma, which can take different forms. Poverty, violence, and inequality are the most common reasons individuals develop risky behaviors and mental health conditions, which is why treating and managing mental health is challenging.
Transgender Mental Health Services & Support Options
Immediate Transgender-Affirming Crisis Hotlines
Hotlines provide immediate free counseling, support, and information to callers. While some hotlines are telephone-only, many are available over text message and online chat.
Hotlines are confidential, but not anonymous unless specified otherwise. This means hotlines will use non-consensual active rescue to send emergency personnel to your location if they believe you are in imminent risk.
These services are best for crises, but are not ideal for long-term counseling. Hotlines are designed to help callers get through severe moments of distress, but are not equipped to manage mental health conditions beyond immediate crises.
Many hotlines are available 24/7, although this depends on agency size and funding. Here are curated directories of LGBTQIA+-affirming hotlines.
Support groups are recurring gatherings of individuals experiencing common issues like depression, substance misuse, and grief. Rather than seeking support solely from therapists, support groups provide people with encouragement, comfort, and connection from peers.
Support groups are frequently the most cost-effective therapy option, often free or low-cost. Unlike hotlines, support groups are a great option to manage mental health long-term because individuals obtain treatment through regular meetings.
These groups offer safe spaces to learn coping skills and self-care. However, they’re not for everyone. Each support group is run differently, but all groups should have clear rules and personal boundaries to allow everyone to share, feel at ease, and stay on topic.
Find a Transgender-Friendly Support Group
Interested in joining a support group? Use these tools to find a group near you.
Mutual support groups are peer-led. Groups are led by members, who are trained to be facilitators, but do not give professional advice.
Mutual support groups are the most casual type of support group. Although they cannot give professional medical advice, these settings allow individuals to share their experiences on what has worked best for their journey. Based on their organization, mutual support groups are almost always free to join.
12-Step Programs for Transgender Recovery
12-step programs use the original support group formula developed by Alcoholics Anonymous to connect individuals in peer-led groups without a professional facilitator. Although 12-step programs are associated with substance misuse, many programs exist for other mental health concerns.
Like mutual support groups, 12-step programs are free for individuals to join. However, 12-step programs utilize religion as a core aspect of programming.
Provider-Led Therapy Groups
Therapy groups are led by a mental health provider who connects individuals with similar struggles. Since therapy groups are facilitated by providers, they can provide professional counseling in a group setting. Individuals can obtain diagnoses and professional treatment without going to individualized therapy.
Some therapy groups are offered for free, but many cost a small fee. Group therapy is always cheaper than individualized sessions.
Virtual & Online Support Groups
Online support groups connect individuals through video calls and messaging rather than physical locations. Some groups may be peer-based similar to mutual support groups, while others may be facilitated by a mental health provider like therapy groups.
Similar to their traditional counterparts, many online support groups are free. Peer-based groups offer free membership, while online therapy groups require a small fee to offset the cost of professional care provided.
Telehealth Counseling & Virtual Therapy
You can receive professional counseling through a cell phone, computer, or other device connected to the internet. Historically, individuals had to visit counselors in person for therapy; the use of telemedicine allows users to access treatment remotely. Unlike online support groups, telehealth counseling connects people to one-on-one sessions with a trained professional.
Some individuals thrive with telehealth therapy. Some are unable to mesh well on a digital platform or obtain the level of support they need without in-person care. Always research your provider since some individuals operate via online platforms without licenses.
Telehealth therapy is not necessarily cheaper than traditional counseling. Telehealth provides more options, but the cost is based on insurance coverage. The best way to find a provider compatible with your healthcare coverage is through ZocDoc, although other platforms accept insurance.
Find a Transgender-Friendly Virtual Therapist
Interested in finding a telehealth counselor? Use these tools to find a professional for you.
Talk therapy provides clinical mental health treatment with a licensed professional to work through long-term issues. Unlike telehealth, traditional counseling requires individuals to visit providers in person.
When searching for a therapist, you should keep licensure, insurance coverage, and relatability in mind.
Every state has a list of requirements mental health professionals must complete to become licensed.
It is possible to find counselors who provide treatment without a license. This is not advised since licensure ensures your counselor is qualified and up-to-date on inclusive and effective treatment methods.
Medicaid, Medicare, and commercial healthcare insurance companies require treatment to be performed by a licensed entity to be covered.
Cost is a barrier for many. To lower the price of treatment, you need to make sure your coverage is compatible.
Health professionals only accept specific coverage plans based on contracts their agency has signed. For your therapy to be covered, you need to find a counselor deemed “in-network” within those contracts. Most providers will have a published list of what coverage plans they accept.
Even if your provider is in-network, more restrictions may apply. Some insurance plans only cover a set number of sessions or pay a portion of the overall fee.
Without healthcare coverage, you will be expected to pay for each visit. Some counselors offer sliding scales for individuals paying out-of-pocket to cut down costs.
To find value and meaningful connection in therapy, you need to be able to connect with your therapist.
Counselors specialize in certain fields. Based on their education, they may have more experience in CBT, psychotherapy, mindfulness, or humanistic approaches.
A counselor’s background will determine whether they focus on specific topics, like religion, LGBTQIA+ issues, depression, or relationships. One therapist may be experienced in grief, while another is well-versed in PTSD.
There is no singular approach or counselor that is right for everyone. Approaches that work for one person may be terrible for others, as frustrating as it may be.
Find a Transgender-Friendly Therapist
Interested in finding a traditional counselor? Use these tools to find a professional for you. Alternatively, the Department of Health and Human Services maintains the HRSA Data Warehouse to direct users to federally funded clinics that provide therapy to low-income individuals.
Self-care isn’t just treating yourself; it is an active commitment to take care of yourself. If you don’t practice physical and emotional self-care, you will eventually burn out. It’s harder than it sounds.
Best self-care practices look different for each person. Your needs are shaped by your background, culture, and experiences: fancy chocolates and bath bombs might be great self-care for one person, whereas someone else might thrive on jogging and talking with loved ones. That’s normal!
Create a solid self-care plan to promote better mental health. Even if you’re unable or don’t want to seek professional treatment, self-care is a great DIY approach to mental health:
Are you taking care of your physical body? This includes taking your prescription medication, drinking enough water, and getting out to exercise.
Are you setting professional boundaries and goals at work? It’s okay to say no to avoid overcommitment, lean on others for support, and know your limits.
Are you in a healthy environment? It’s difficult to stay healthy if you live in a polluted neighborhood or drink dirty water. Clean up your living spaces to be organized, fresh, and greener – or get involved with your community to volunteer.
Are you financially healthy? Income uncertainty causes stress. Check your spending habits, set realistic goals, and start saving.
Are you maintaining good relationships? You’re not obligated to keep toxic friendships. Spend time with others face-to-face and online in balanced moderation.
Are you keeping your mind active? Build skills by reading interesting topics, watching new documentaries, or take one of your hobbies to the next level.
Are you emotionally healthy? Practice mindfulness by reaching out to mentors and friends about your struggles, going for a walk, or meditating.
Are you taking care of your fundamental values and goals? Even if you’re not religious, reflect on your current life position, whether you’re content, and where you want to be in the future.
Find things that calm you. Self-care only works if you enjoy what you’re doing. Most people suggest journaling and meditation, but self-care can be ANYTHING. Self-care can be listening to music, drawing, making bracelets, watching a comfort show, or playing video games.
Create a list of your current coping skills. These are habits to utilize when experiencing stressful situations. Expand your list and work on cutting out negative coping mechanisms. Unhealthy coping skills manage emotions, but negatively impact our lives. Unhealthy coping skills include things like substance abuse, anger outbursts, overworking, and self-harm.
There are five types of positive coping skills. No skill is inherently superior or better. It’s best to learn about several types and include any that work to your mental health toolbox.
Problem-based coping skills force you to actively identify stressors, create ideas on how to change your circumstances, and take action with reasonable solutions.
Emotion-based coping skills process emotions and work to reduce internal distress by reframing thoughts. These skills are especially helpful when encountering situations you can’t control.
Religion-based coping skills use rituals like prayer to deal with stressors. By feeling connected to a higher power, individuals can relieve anxiety.
Meaning-making coping skills reframe stressful situations for silver linings. When we can find meaning in our experiences, we find purpose despite stress and danger.
Social support coping skills connect us to mentors, friends, and peers. Talking with support systems reduces stress, whether it’s feeling less alone by going to a support group or feeling valued after cooking a meal for a neighbor.
It is important to maintain a range of coping skills. There is no singular type that is perfect for all scenarios, and all coping skills can become negative if not practiced in moderation. Too much time spent on emotion-based skills makes people too reluctant to change situations where they can make a difference; too much religion-based coping becomes negative when folks put off dealing with problems by staying it’s God’s will.
Example of Coping Skills in Action
Tristan opens an email to find his annual performance review. He is surprised to see that the review states he is below average in several areas, even though he thought he had been performing well. Tristian becomes anxious and frustrated.
Problem-Based Approach
Tristan goes to his boss to discuss what he can do to improve his job performance. It makes him nervous to talk to her directly about it, but they develop a clear plan. Tristian feels confident about his ability to succeed.
Emotion-Based Approach
Tristian spends his lunch break reading a book to distract himself from making catastrophic predictions that he will be fired. After work, Tristian exercises and plays video games as a way to feel better. Tristian feels he can think about the situation more clearly.
Religion-Based Approach
Tristian goes to his local church after work. Tristian prays, reflecting on his purpose and relationships with a higher power by talking to his pastor. Tristian feels less anxious.
Meaning-Making Approach
Tristian spends time thinking about silver linings after work. He reflects on the meaning of his work and whether it makes him feel fulfilled. Thinking about his job options makes Tristian feel empowered to make new decisions to impact his life.
Social Support Approach
Tristian meets with friends after work for dinner. He vents about the review and emotions he is experiencing. His friends alleviate his fears of being fired and give advice on how to best improve his performance. Tristian feels supported by his loved ones.
Find Transgender-Friendly Self-Care Tools
Interested in learning more about self-care? Use these recommended apps and tools to practice self-care in your life.
How to Create a Personal Mental Health Safety Plan
Safety plans are pre-written personalized strategies to use when one is struggling with stressors. During a crisis, it is difficult to think of healthy coping mechanisms. Download Trans Soliary Project’s safety plan or create one with MySafetyPlan.org.
There are three things to remember when crafting your personal safety plan.
Keep it doable. For your safety plan to work, you need it tailored to what suits you. Don’t put overly complex warning signs or coping skills too difficult to use in a crisis.
It’s not written in stone. Writing down a skill isn’t a mandate. Your safety plan should be flexible; you can add or change items as needed.
It doesn’t have to be completed in one sitting. Safety plans take a lot of emotional energy, so it’s natural to need a break before completing them. Complete as much as possible and come back to it later.
Identifying Your Mental Health Warning Signs
Warning signs are thoughts, actions, and places that trigger a mental health crisis. Developing the ability to identify warning signs allows you to know when to use your safety plan best. The goal is to engage in positive coping skills when you first notice warning signs to avoid spiraling.
Common warning signs include:
Feelings of hopelessness
Feeling the urge to cry
Feeling the urge to self-harm
Isolating yourself
Having intrusive thoughts
Not eating
Racing heart or shaking
Mood swings, anger, and agitation
Increased alcohol or drug use
Neglecting personal care or hygiene
The key is to identify signs you experience before you feel suicidal or the urge to self-harm. It’s easier said than done. Always use caution to avoid overwhelming yourself as you complete this step.
Choosing Immediate Crisis Coping Strategies
Coping strategies are actions you can complete to feel better in a moment of stress. Coping strategies might not make you feel perfect, but the goal is to move out of crisis.
Emotion-based coping skills are ideal in a crisis. When experiencing immense stress, it is better to reduce distress rather than hyperfixate on solutions to break out of the spiral.
Common positive coping strategies include:
Watching funny or inspirational videos
Journaling or writing poetry
Listening to music
Doing a puzzle
Playing video games
Drawing, painting, or another artistic hobby
Going for a walk or run
Spending time with a pet
Writing down positive affirmations
Mindful meditation and grounding exercises
There are hundreds of coping skills. Pick out at least ten that revolve around hobbies and activities you genuinely enjoy. Keep these strategies doable, since you will be attempting them while potentially experiencing a mental health crisis.
Building Your Personal Support Network
Supports are individuals you feel safe and comfortable enough around to tell when you are experiencing suicidal thoughts or urges to self-harm. To be effective, these individuals can’t be people you would feel embarrassed having tough discussions with.
List at least three people that you trust to support you in a crisis. These can be family members, a close friend, a partner, a mentor, or even a higher power. Prioritize individuals who make you feel good. It is important to list more than one person in case they’re busy or unreachable while you’re in distress.
Identifying Professional Crisis Resources & Agencies
Professionals are individuals and agencies you can contact when coping strategies and supports aren’t enough to bring you out of crisis. These include therapists, crisis hotlines, urgent care teams, and emergency rooms.
At this point, you may need inpatient treatment at a psychiatric hospital if you are in danger of harming yourself or others. Most hotlines and professional agencies use nonconsensual rescue if they genuinely believe you may kill yourself. Go through our hotline directories here.
Modifying Your Physical Environment for Safety
It is important to consider potential dangers in your regular environment if you are experiencing mental health concerns. What can you do now to limit your access to threats later?
Limit access to firearms, sharp objects, lighters, and drugs. Expand your ability to access previously listed tools, like having a backup phone or wifi connection. Have an open conversation with those you live with that you’re taking an active approach to your mental health. They can also help implement your safety plan.
Final Steps: Implementing Your Safety Plan
Safety plans are versatile and can include non-mental health crises. You can include local homeless shelters, fire departments, law enforcement, health departments, or anything else you feel would be helpful. Each person and every crisis is unique.
Lastly, write down at least five reasons for living. These can be goals, photos, or objects – it doesn’t matter how small these reasons might seem. Any reason that keeps you alive is worth writing down, regardless of whether it’s a person or pet you love, a TV show you want to finish, or a concert you want to see one day.
Once completed, download an electronic copy of your safety plan to easily access on your phone. Keep additional copies on a computer or online, like Google Drive or iCloud.
Looking for more resources?
Browse Trans Solidarity Project’s resources, or check out these posts:
Human Immunodeficiency Virus (HIV) is a virus that attacks CD4 white blood cells, gradually weakening the body’s immune system over time. Although there is currently no cure, HIV has been a manageable chronic condition since 1996.
What’s the difference between HIV and AIDS?
Acquired Immunodeficiency Syndrome (AIDS) is the final and most severe stage of HIV if left unmanaged. When HIV progresses to AIDS, the body’s immune system is badly damaged to the point that it can’t fight off normal infections.
In the United States, most people with HIV do NOT develop AIDS. Taking HIV medication (Antiretroviral Therapy) halts HIV from progressing or further damaging CD4 cells.
How is HIV Transmitted?
You can only give HIV by coming in contact with certain bodily fluids from a person with a detectable HIV viral load. These fluids include:
Semen
Pre-Seminal Fluid
Blood
Rectal Fluid
Vaginal Fluid
Breast Milk
HIV can NOT be spread by kissing, hugging, or sharing food. Behaviors that put you at higher risk of HIV include anal sex, vaginal sex, and sharing needles. Kissing and oral sex have statistically nonsignificant chances of transmitting the human immunodeficiency virus.
US Centers for Disease Control and Prevention. Use the HIV Risk Reduction Tool to learn about your risk for HIV based on behaviors and practices.
What Does Viral Load Mean?
The term “viral load” refers to how many copies of the human immunodeficiency virus someone has. HIV is diagnosed once someone has more than 200 copies of human immunodeficiency virus per milliliter of blood.
Individuals with a viral load of 200 or more can transmit HIV to other people. Since their viral load can be detected on most HIV tests, we refer to these as “detectable” viral loads.
Undetectable viral loads refer to individuals living with HIV who have FEWER than 200 copies per milliliter. Due to the low copy count, these individuals can test negative on HIV tests and are hence “undetectable.” People with undetectable viral loads have effectively no risk of transmitting HIV to other people, even without regular precautions like condoms, PEP, and PrEP. Undetectable viral loads are achieved by taking antiretroviral therapy medication regularly.
What Are Symptoms of HIV?
The only way to know your HIV status for sure is to get tested. Despite misconceptions, you cannot tell if someone has HIV just by looking at them. Most people with HIV do not experience major symptoms.
In symptomatic individuals, HIV often causes flu-like symptoms while in its earliest stages. Within two to four weeks of HIV infection, two-thirds of people may experience:
Fever
Chills
Rash
Night Sweats
Muscle Aches
Sore Throat
Fatigue
Swollen Lymph Nodes
Mouth Ulcers
HIV can be detected 10 to 33 days after infection. Remember that PEP can prevent HIV up to three days after infection exposure.
After the first four weeks, HIV enters its chronic latency stage. Flu-like symptoms vanish as the virus multiplies over the next 10 to 15 years. Without medication intervention, chronic HIV progresses to AIDS. Individuals with AIDS can also live long lives with consistent medication, but life expectancy drops to three years without intervention.
Who Is at Risk of HIV?
Anyone can get HIV. HIV does not discriminate based on sexual orientation, gender identity, race, ethnicity, age, or neighborhood. However, some groups of people are considered high-risk.
Men who have sex with men (MSM, queer men, bi+ men) account for 65% of new HIV diagnoses. Conversely, 22% of new diagnoses come from straight individuals engaging in heterosexual sex.
Individuals who inject drugs and share needles account for 7% of new HIV diagnoses annually.
Most new HIV diagnoses come from individuals between the ages of 25 and 34. The second-highest age group is 24 and under, who made up 20% of new diagnoses in 2022.
How Do I Prevent HIV?
There are many ways to prevent HIV. By learning how to prevent HIV transmission, you’re helping end the HIV epidemic. The most common ways to prevent HIV include condom use, PEP, PrEP, scheduled wellness testing, and limiting needle/drug equipment sharing.
US readers should visit HIV.gov for official HIV-related care and prevention practices.
What Are PEP & PrEP?
Post-exposure prophylaxis (PEP) is an anti-HIV medication started within 72 hours of possible HIV exposure. It is taken daily for 28 days and followed up with additional testing and labs for the next three months. The sooner PEP is started after possible infection, the more effective it will be.
Pre-exposure prophylaxis (PrEP) is a daily anti-HIV prevention medication that blocks HIV starting seven days of use. PrEP is best for individuals who regularly encounter HIV, like from casual hookups, sharing needles, or inconsistent condom usage.
When taken consistently, PrEP reduces the risk of contracting HIV from sex by 99%. Individuals who share needles see a 74% HIV risk decrease with PrEP use.
PEP is for emergencies, similar to how Plan B and emergency contraception prevent pregnancy after unprotected sex. PrEP is for long-term use, like how birth control pills prevent HIV when taken consistently every day.
Individuals residing in the United States can use PrEP Locator to find local PrEP providers. NASTAD has information regarding whether non-providers (ex. pharmacies) can prescribe PrEP based on state or territory.
How Do I Get Tested For HIV?
Getting tested for HIV can be scary, but remember that HIV is NOT a death sentence. People living with HIV experience long and healthy lives as long as they are connected with the tools necessary to keep their HIV managed. People can only start HIV treatment if they know they are living with the virus, so it’s important to get tested.
The CDC recommends EVERYONE be tested for HIV at least once in their lives. High-risk individuals should get tested at least once annually. It is only recommended to get tested more frequently (ex. every three months) if you are at an extreme risk of getting HIV without preventative medication like PrEP.
Getting tested helps end the spread of HIV. Get tested today to keep yourself healthy and protect those you love from contracting HIV.
Types of HIV Tests
There are three types of HIV tests, which can use blood, saliva, or urine to detect a viral load.
HIV tests search for antibodies and antigens that are only produced when infected with the human immunodeficiency virus. However, it takes time for the body to begin producing these after initial infection. This creates a “window period” between contracting HIV and the earliest time it can show up positive on a test. Some tests have smaller window periods than others.
Antibody tests detect HIV antibodies in the blood or saliva. The majority of rapid HIV tests are antibody tests, including HIV self-test kits.
Antigen/antibody tests look for BOTH HIV antibodies and antigens in the blood. Antigens are proteins created by the virus, appearing much sooner than antibodies. Antigen/antibody tests are the most common HIV test conducted in US labs.
Nucleic acid tests (NATs or viral load tests) detect the amount of HIV present in someone’s blood. NATs are useful to monitor the virus once someone is living with HIV and can detect HIV as soon as 10 days after infection. Nucleic acid tests are significantly more expensive than antibody or antigen/antibody tests, so they’re reserved for HIV management.
How to Get an HIV Test
HIV tests are widely available. You can test at home, a primary doctor, hospital, medical clinic, substance use program, or community health center. HIV self-test kits can even be purchased on Amazon or at Walmart. It’s entirely your choice!
Visit gettested.cdc.gov to find an HIV testing site near you. Together TakeMeHome is a CDC program that provides free rapid self-tests to anyone at least 17 years old in the United States.
What Happens If I Test Positive?
Rapid tests, including at-home kits, are positive if there are two complete lines. Even a faint second line means you may have HIV.
Take a deep breath. You’re not alone. Remember, modern treatments are available to ensure people live long and happy lives with HIV. Having HIV does not mean you have or will have AIDS.
Visit a clinic or healthcare provider to confirm your results with a nucleic acid test.
If your results are confirmed as positive, you will be given resources and information about HIV treatment and management.
You will be connected with case management, including counseling and HIV support organizations.
Healthcare workers are required to keep all medical information confidential unless you give explicit permission otherwise. No one will know about your test or results unless you want them to, including family members or your workplace.
Healthcare providers are required to report positive results to local health departments, but your information will be kept confidential. Health departments can assist individuals anonymously contact sexual partners to inform them of potential exposure, although this is generally not required.
Learning you may have HIV is distressing. OraQuick has a toll-free support line for individuals self-testing, available at 866-436-6527.
What Happens If I Test Negative?
Rapid tests, including at-home kits, are negative if there is one complete line. There should be NO line (however faint) next to “T.”
If your result is negative AND it has been at least three months since your latest possible HIV exposure, you likely do not have HIV. Continue to maintain healthy sexual habits like condom usage, PrEP, and getting tested as needed.
Remember that a negative self-test does not 100% mean you are not infected with HIV. Rapid tests have a larger window period to detect HIV, so it’s possible to get a false negative.
Do People With HIV Have Legal Rights?
Legal rights vary drastically for people living with HIV based on where they are in the world. People with HIV are discriminated against at work, home, and the doctor’s office; knowing your rights is the first step in defending them.
Individuals living with HIV in the United States are protected by the Rehabilitation Act of 1973 and the Americans with Disabilities Act of 1990. These laws are enforced by the Department of Health and Human Services and the Office for Civil Rights to prohibit anti-HIV discrimination by all agencies that receive federal funding.
Insurance companies are not allowed to charge more or deny coverage based on HIV status. The Affordable Care Act prohibits insurance companies from cancelling or rescinding coverage based on pre-existing conditions. Insurance companies are also forbidden from notifying employers of possible HIV status.
Medicaid programs must include HIV treatment. In states without expanded Medicaid, low-income individuals can obtain care through the Ryan White HIV/AIDS Program.
Report agencies violating the Rehabilitation Act or ADA by filing with the Office for Civil Rights.
Employers are not allowed to fire someone because of their HIV status, although small companies with 15 or fewer employees have partial exemptions from the ADA. Employers may only ask standard medical questions related to the core functions of the job. While an employer can refuse to hire someone if they pose a direct health threat, they cannot deny an HIV-positive individual if the risk can be managed with reasonable steps.
Employers are not allowed to tell others about your HIV status. You are not required to disclose your status to your employer, but employers aware of your status are required under the ADA to keep HIV-related information confidential.
Your HIV status is considered personal medical information, so you have the right to keep it private and confidential. HIPAA prohibits healthcare providers from telling others your status without your explicit consent.
Public accommodations that offer goods and services to the public cannot discriminate against people with HIV. This includes restaurants, hotels, stores, gyms, and private schools. These protections also extend to government services and buildings. Private clubs and certain religious organizations are NOT considered public accommodations and are therefore exempt.
The Fair Housing Act prevents anti-HIV discrimination in housing. Landlords are not allowed to refuse to rent, charge more, or evict someone based on HIV status. Landlords also aren’t allowed to ask about the nature or severity of someone’s HIV status or refuse to make reasonable accommodations.
13 states require individuals to disclose their HIV status to current and new sexual partners. Only two states (Indiana and North Carolina) require individuals to inform previous sexual partners of their HIV status. The type of sexual contact that triggers disclosure obligation varies from state to state.
You may have a legal obligation to disclose your HIV status when donating blood/organs/tissue, or sharing injection drug equipment. Arkansas is currently the only state that requires individuals to disclose their HIV status when visiting a physician or dentist in-state.
Having HIV does not impact your ability to care for or adopt children. HIV status alone cannot affect child custody.
HIV status cannot create additional barriers to immigration into the United States. Individuals living with HIV may obtain political asylum in the US if they can prove fear of persecution in their country of origin. Immigration detention facilities are required to have access to health care services, including HIV prevention, diagnosis, and treatment.
AIDS Healthcare Foundation @ aidshealth.org / 323-860-5200 / International nonprofit based in Los Angeles that operates a network of HIV services in over 40 countries across Latin America, Africa, Asia, and Europe.
International Planned Parenthood Federation @ ippf.org / 202-987-9364 / Global healthcare provider that has been a leader in sexual and reproductive health for all since 1952.
UNAIDS @ unaids.org / 41-22-595-59-92 / International agency that seeks to end AIDS as a public health threat by 2030 and has operated since 1996 to assist the United Nations in combating HIV and AIDS.
HIV Hotlines in North America
Canada
Canadian AIDS Treatment Information Exchange @ catie.ca/ 416-203-7122 / The primary national information and resource center on HIV, Hepatitis C, and substance misuse in Canada.
HIV and Sexual Health Infoline Canada @ sexualhealthontario.ca / 800-668-2437 / Free anonymous telephone and instant message service available in English and French on sexual health topics. Advice and counseling can be available for any Canadian resident, although services are specified for Ontario.
LGBT National Help Center @ lgbthotline.org / 888-843-4564 /Free and confidential peer-suppor on gender and/or sexuality, crisis prevention, and community connections. Maintains a coming out hotline, youth talkline, and senior hotline. Also maintains LGBTnearMe.org and LGBTPridePath.org.
Trans Lifeline @ translifeline.org / 877-565-8860 / Transgender-centered crisis organization that does not use involuntary intervention/forced hospitalization to provide support to transgender people through fully anonymous and confidential calls within the United States and Canada.
Jamaica
National HIV/STI Helpline @ hstu.moh.gov.jm / 876-536-9141 / Program under the Ministry of Health and government of Jamaica to implement and support HIV/AIDS response in the nation.
Mexico
The Trevor Project @ thetrevorproject.mx / 52-55-9225-3337 / The leading suicide prevention and crisis intervention organization centered on LGBTQIA+ young people in Mexico. Offers 24/7/365 information and support to those ages 13 to 24 with trained counselors via WhatsApp and instant message.
United States
CDC-INFO @ cdc.gov / 800-232-4626 / Live support to help Americans find the latest and reliable science-based health information, including CDC guidance and resources.
HIV/AIDS/Hepatitis C Nightline / 800-273-2437 / US hotline providing support for people living with HIV or Hepatitis C as well as their caregivers.
HIV Management Warmline / 800-933-3413 / Non-emergency telephone service for questions about HIV, antiretroviral therapy, HIV clinical trials, and laboratory evaluation in the United States.
LGBT National Help Center @ lgbthotline.org / 888-843-4564 /Free and confidential peer-suppor on gender and/or sexuality, crisis prevention, and community connections. Maintains a coming out hotline, youth talkline, and senior hotline. Also maintains LGBTnearMe.org and LGBTPridePath.org.
National AIDS Hotline / 800-243-2437 / Federal hotline to refer the general American public to relevant state and local resources.
National AIDS Treatment Advocacy Project @ natap.org / 212-219-0106 / Nonprofit corporations in the United States that educates individuals on HIV treatments on the local, national, and international level.
National Clinician Consultation Center @ nccc.ucsf.edu / 833-622-2463 / Teleconsultation resource that educates US healthcare providers with information and answers on HIV and Hepatitis C.
NIH Office of AIDS Research @ hivinfo.nih.gov / 800-448-0440 / Confidential answers to questions on HIV/AIDS clinical trials and treatment in the United States.
PEPline / 888-448-4911 / Hotline for individuals interested in information about PEP, especially those who have been possibly exposed to HIV while on the job in the United States.
PrEPline / 855-448-7737 / Hotline about how to start, continue, or manage use of PrEP for HIV within the US.
SAGE x HearMe @ sageusa.org / The United States’ largest and oldest organization dedicated to improving the lives of LGBTQIA+ older people. SAGE now offers supportive services and resources through the SAGE x HearMe app, formerly known as the SAGE LGBTQ Elder Hotline.
The Trevor Project @ thetrevorproject.org / 866-488-7386 / The leading suicide prevention and crisis intervention organization centered on LGBTQIA+ young people in the United States. Offers 24/7/365 information and support to those ages 13 to 24 with trained counselors via call, text, or instant message.
Trans Lifeline @ translifeline.org / 877-565-8860 / Transgender-centered crisis organization that does not use involuntary intervention/forced hospitalization to provide support to transgender people through fully anonymous and confidential calls within the United States and Canada.
HIV Hotlines in Europe
France
Sida Info Service @ sida-info-service.org / 0-800-840-800 / Free confidential telephone service for anyone in mainland France or in affiliated overseas departments to get information regarding HIV. Callers from outside France should dial 00-31-1-41-83-42-77.
Germany
AIDS-Hilfe Helpline @ aidshilfe.de / 0180-33-19411 / Telephone counseling provided via the telephone that answer provides information in Germany on HIV/AIDS.
Russia
HIV Hotline @ стопвичспид.рф/ 8-800-555-49-43 / Hotline operated in conjunction with Russia’s STOP HIV/AIDS campaign to answer questions about HIV.
United Kingdom
Terrence Higgins Trust @ tht.org.uk / 0808-802-1221 / Telephone and live chat service for individuals residing in the United Kingdom seeking support and information about HIV.
HIV Hotlines in Asia
Hong Kong
AIDS Hotline / 852-2780-2211 / Counseling staffed by trained nurses for information about HIV and testing in Hong Kong.
Gay Men HIV Testing Hotline / 852-21171069 / Free anonymous and confidential HIV testing service provided in Hong Kong by appointment and telephone.
India
National AIDS Control Organization Helpline @ naco.gov.in / 1097 / National Indian helpline that provides counseling and awareness on HIV/AIDS prevention, treatment, and education.
Israel
AIDS Task Force @ aidsisrael.org.il / 03-5619900 / Telephone and WhatsApp service for individuals in Israel seeking support and resources about HIV and AIDS.
Philippines
National HIV and AIDS Hotline @ pnac.doh.gov.ph / 632-8-651-7800 (Local 2283) / National telephone support line for HIV and AIDS information in the Philippines, provided by the Department of Health and Philippine National AIDS Council. PNAC can also be reached by email via secretariat@pnac.gov.ph, Facebook, or TikTok at @pnac11166.
Russia
HIV Hotline @ стопвичспид.рф/ 8-800-555-49-43 / Hotline operated in conjunction with Russia’s STOP HIV/AIDS campaign to answer questions about HIV.
Türkiye
Positive Living Association @ pozitifyasam.org / 0216-418-10-61 / Support line in Türkiye to make up-to-date information about HIV accessible and connect people with relevant testing and prevention services.
HIV Hotlines in Africa
Kenya
National HIV and AIDS Helpline @ nhcsc.nascop.org / 0726-460-000 / Hotline operated by the National HIV Clinical Support Center to advise individuals in Kenya about HIV/AIDS.
Nigeria
AIDS Helpline / 234-01-772-2200 / Toll-free hotline system for accurate and up-to-date information about HIV/AIDS in Nigeria.
South Africa
National AIDS Helpline @ lifelinesa.co.za / 0800-012-322 / Emotional support counseling for HIV/AIDS in South Africa.
Uganda
AIDS Information Centre @ aicug.org/ 256-39-3101893 / Healthcare network that leads HIV/AIDS treatment, prevention, and counseling throughout Uganda.
HIV Hotlines in Oceania
Australia
National HIV/AIDS Information Line / 1800-451-624 / Advice line that connects individuals to qualified sexual health nurses in Australia for confidential information about HIV, operated by the Sexual Health Info Link.
New Zealand
Burnett Foundation @ burnettfoundation.org.nz / Free and confidential counseling for people living or affected by HIV in New Zealand, available by appointment.
HIV Organizations & Tools
International HIV Organizations & Tools
Global Network of People Living with HIV @ gnpplus.net / Network operated by people living with HIV for people living with HIV, regardless of geographic location.
International AIDS Society @ iasociety.org / Research-based organization that develops holistic approaches to HIV/AIDS treatment and prevention.
International Planned Parenthood Federation @ ippf.org/ Global healthcare provider that has been a leader in sexual and reproductive health for all since 1952.
The Global Fund to Fight AIDS, Tuberculosis, and Malaria @ theglobalfund.org / Worldwide partnership to combat HIV, tuberculosis, and malaria and create healthy, safe, and equitable communities.
UNAIDS @ unaids.org/ International agency that seeks to end AIDS as a public health threat by 2030 and has operated since 1996 to assist the United Nations in combating HIV and AIDS.
HIV Organizations & Tools in North America
Canada
Canadian Aboriginal AIDS Network @ caan.ca / Agency in Canada that provides resources and tools to Indigenous and Aboriginal Canadians.
Canadian AIDS Society @ cdnaids.ca / Grassroots network that leads community-based HIV/AIDS resources in Canada.
Canadian AIDS Treatment Information Exchange @ catie.ca/ The primary national information and resource center on HIV, Hepatitis C, and substance misuse in Canada.
Canadian HIV/AIDS Legal Network @ hivlegalnetwork.ca / Network that promotes the human rights of people living with HIV/AIDS across Canada, which includes legal representation and legislation advisement
United States
AIDS Drug Assistance Program@ adap.directory / Patient-centric project that provides HIV-related services and prescription medication to hundreds of thousands of people in the United States by linking individuals with their local state or territory agency.
Asian Pacific AIDS Intervention Team @ apaitssg.org/ Grassroots AIDS service organization centered on Asian and Pacific Islanders with HIV, based in the United States.
Bienestar Human Services @ bienestar.org / US community-based social services organization that caters to Latino Americans living with HIV, especially LGBTQIA+ Latino Americans.
Black AIDS Institute @ blackaids.org / Think tank that aims to end the HIV/AIDS epidemic in the Black American community through awareness messaging, information, and robust programs.
HIV.GOV @ hiv.gov / Offers information about HIV/AIDS prevention, treatment, and resources for anyone in the United States.
HIV.GOV Service Locator @ locator.hiv.gov / Location-based search tool managed by the United States Department of Health and Human Services to allow anyone to find local HIV testing services, housing providers, health centers, PrEP, PEP, and other related needs.
Latino Commission on AIDS @ latinoaids.org / Nonprofit organization in response to the critical unmet need for HIV prevention, treatment, and education in the Latino community in the United States.
National Minority AIDS Council @ nmac.org / Advocacy nonprofit that provides training and resources catered to marginalized communities in the United States.
National Native HIV Network @ nnhn.org / Indigenous-led network that mobilizes American Indians, Indigenous Americans, Alaska Natives, and Native Hawaiians towards community action.
Positively Trans @ transgenderlawcenter.org / Program through the Transgender Law Center to support transgender people living with HIV in the United States.
Positive Women’s Network @ pwn-usa.org / Advocacy and resource organization for women living with HIV.
Ryan White HIV/AIDS Program @ ryanwhite.hrsa.gov / National services and resources for low-income individuals living with HIV in the US.
TheBody.com Hotline @ thebody.com / News site based in New York that centers on publishing HIV-related information.
The Well Project @ thewellproject.org / United States nonprofit that primarily supports women and girls living with HIV/AIDS.
HIV Organizations & Tools in South America
RedLA+ @ redlactrans.org / Network of organizations that focus on transgender people throughout Latin America, especially those who are living with HIV.
HIV Organizations & Tools in Europe
AIDS Action Europe @ aidsactioneurope.org/ Regional network of over 370 NGOs, national networks, and community-based groups to support legislation related to HIV/AIDS in 47 different countries.
European AIDS Treatment Group @ eatg.org/ Advocacy and research organization that responds to and develops HIV/AIDS-related initiatives.
United Kingdom
National AIDS Trust @ nat.org.uk / The primary HIV rights charity in the United Kingdom.
HIV Organizations & Tools in Asia
Asia Pacific Network of People Living with HIV @ apnplus.org / Peer-led organization that improves the quality of life for people living with HIV/AIDS in the Asia Pacific region.
Middle East and North Africa Harm Reduction Association @ menahra.org / Network of HIV/AIDS prevention and treatment organizations in 20 different countries across the Middle East and Northern Africa.
India
India HIV/AIDS Alliance @ allianceindia.org / Non-governmental organization that partners with various civic society, government, and community groups to support HIV prevention and treatment programs.
Thailand
MPlus Foundation @ mplusthailand.com/ Community-based sexual health and rights organization based in Thailand that works to end HIV discrimination and transmission.
Thai Red Cross AIDS Research Centre @ trcarc.org / Research organization and health clinic that serves individuals with HIV/AIDS in Thailand.
HIV Organizations & Tools in Africa
African Network for the Care of Children Affected by HIV/AIDS @ anecca.org / Reproductive health organization that serves people living in Uganda, Burundi, Ethiopia, Nigeria, Malawi, Tanzania, and South Sudan.
Middle East and North Africa Harm Reduction Association @ menahra.org / Network of HIV/AIDS prevention and treatment organizations in 20 different countries across the Middle East and Northern Africa.
South Africa
Desmond Tutu HIV Foundation @ desmondtutuhivfoundation.org.za / Health organization that partners with various international research groups to develop community programs in South Africa.
Treatment Action Campaign @ tac.org.za / Civic society organization based in South Africa that leads campaigns centered on improved healthcare for people living with HIV/AIDS.
HIV Organizations & Tools in Oceania
Australian Federation of AIDS Organizations @ healthequitymatters.org.au/ Federation of HIV and LGBTQIA+ organizations in Australia and Oceania that provides policy expertise and resource support.
Pacific Sexual and Gender Diversity Network @ psgdn.org / Collective between the countries of Fiji, Samoa, and Tonga to advocate for the needs of people living with HIV, especially LGBTQIA+ people.
New Zealand
Burnett Foundation @ burnettfoundation.org.nz / Formerly known as the New Zealand AIDS Foundation, the Burnett Foundation Aotearoa is a community-led response organization that tackles HIV throughout New Zealand.
Frequently Asked Questions
Don’t only gay men get HIV?
No. Although men who have sex with men (MSM) have historically had higher infection rates, anyone can be infected with HIV.
According to the CDC, 22% of new HIV diagnoses in the United States are heterosexual.
Wouldn’t I know if I had HIV?
You can’t tell someone has HIV based on appearances. Most people living with HIV do not experience major symptoms.
1 in 7 people diagnosed with HIV had no idea that they were carrying the virus. It’s incredibly important to test regularly if you engage in high-risk behaviors like injectable drugs or frequent sexual partners.
Won’t HIV kill you?
No. People living with HIV can live long, healthy lives just like everyone else as long as they are managing their HIV with medication. HIV only becomes deadly if left undiagnosed or untreated.
Isn’t it OK to have unprotected sex if both partners have HIV?
No. Unprotected sex is still risky, even if all partners involved have HIV. You can still get other STDs like chlamydia, gonorrhea, syphilis, and other strains of HIV.
Doesn’t birth control prevent HIV?
No. Condoms, PEP, and PrEP are the only ways to prevent HIV infection. Birth control methods like the pill, IUDs, and implants do NOT prevent HIV or other STDs.
There are a handful of experimental HIV vaccines available via clinical trial, such as RV144.
Aren’t HIV-preventative medications too expensive for me?
Many US states and Canadian provinces provide HIV-preventative medication like PEP and PrEP for free. Visit your nearest health department for more information or check out PrEPMAP.




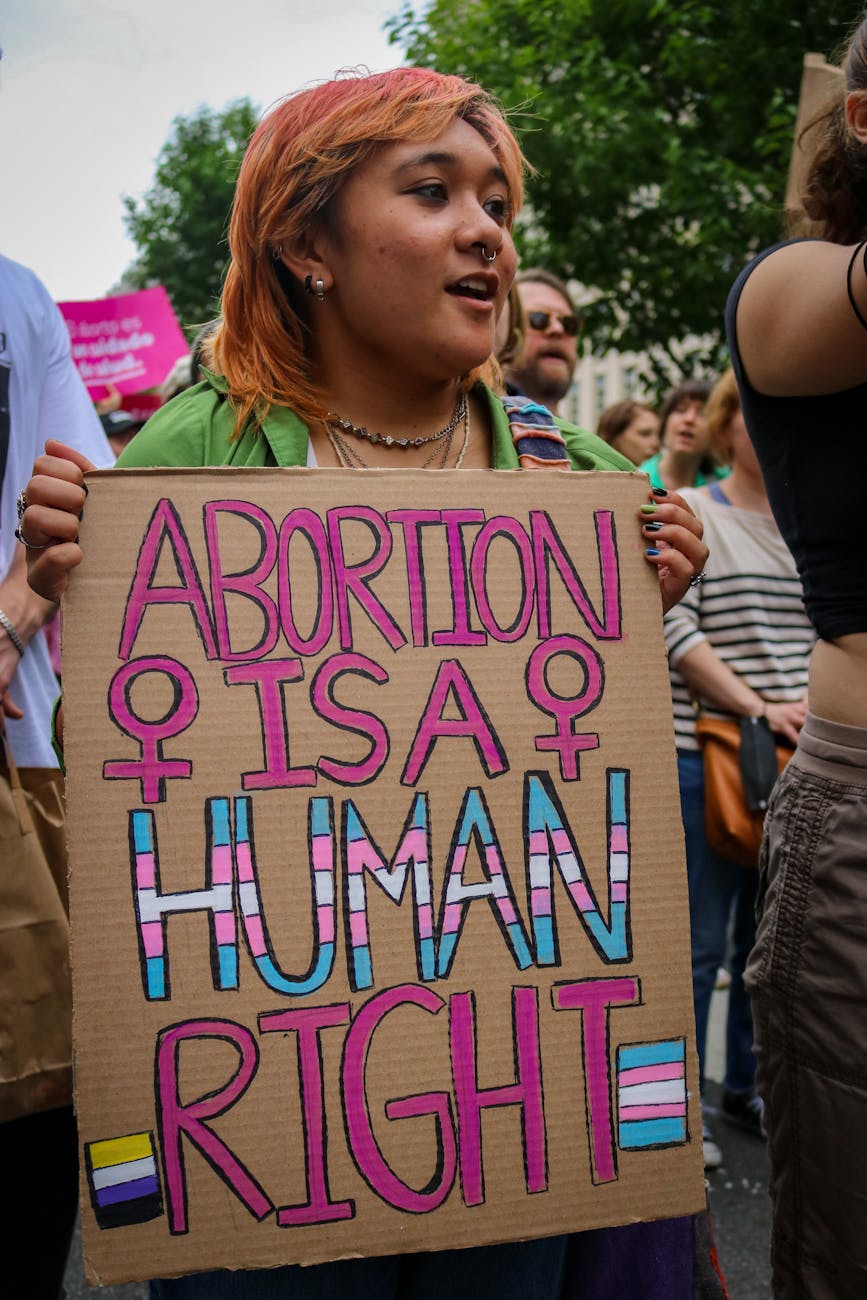














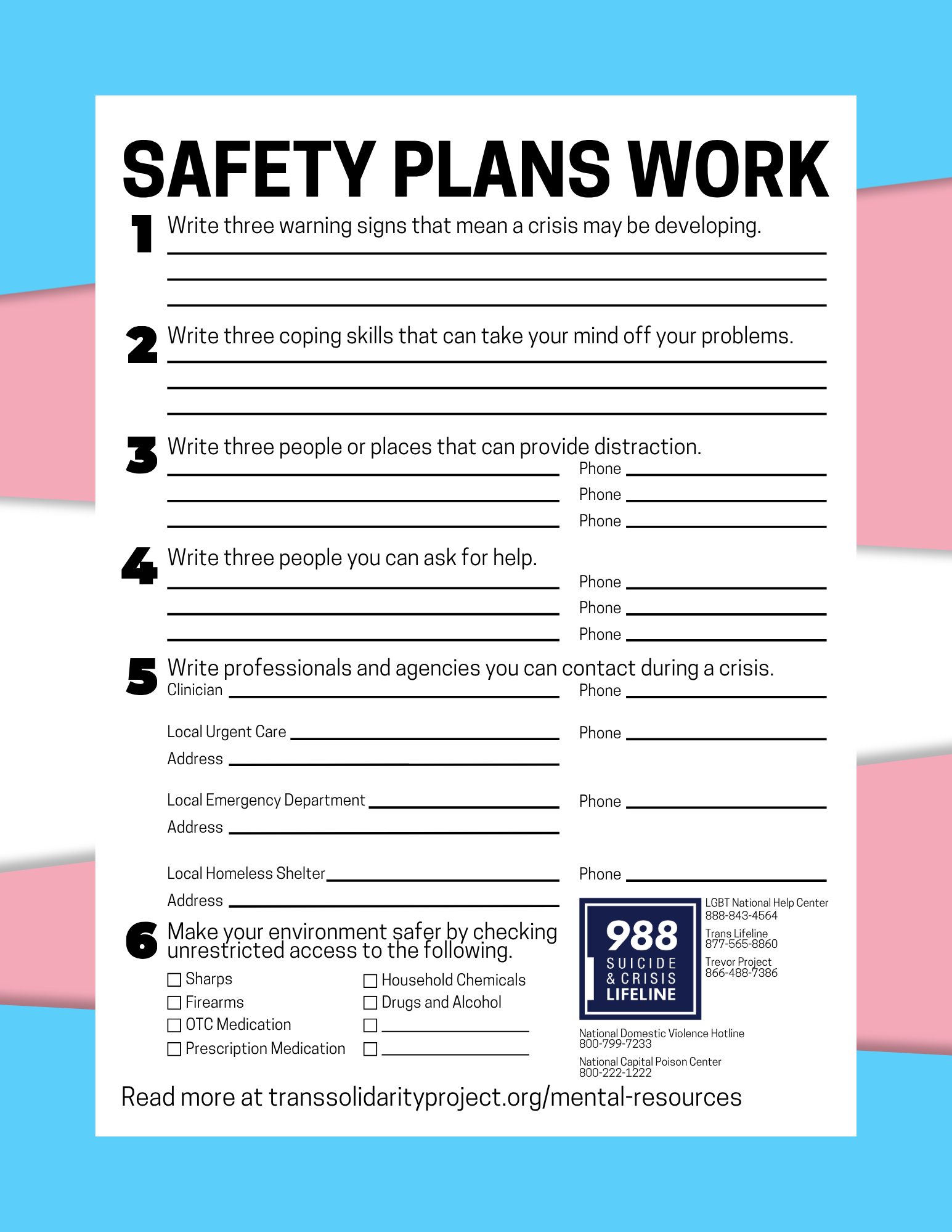{kind=link}